Ran Yuanyuan, Liu Zongjian, Huang Shuo, Shen Jiamei, Li Fengwu, Zhang Wenxiu, Chen Chen, Geng Xiaokun, Ji Zhili, Du Huishan, Hu Xiaoming
1China-America Institute of Neuroscience, Beijing Luhe Hospital, Capital Medical University, Beijing, China.
2Central Laboratory, Beijing Luhe Hospital, Capital Medical University, Beijing, China.
Aging Dis. 2018 Jun 1;9(3):467-479. doi: 10.14336/AD.2018.0130. eCollection 2018 Jun.
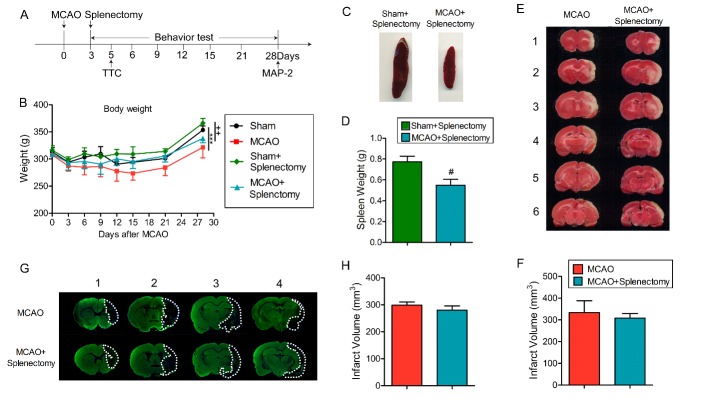
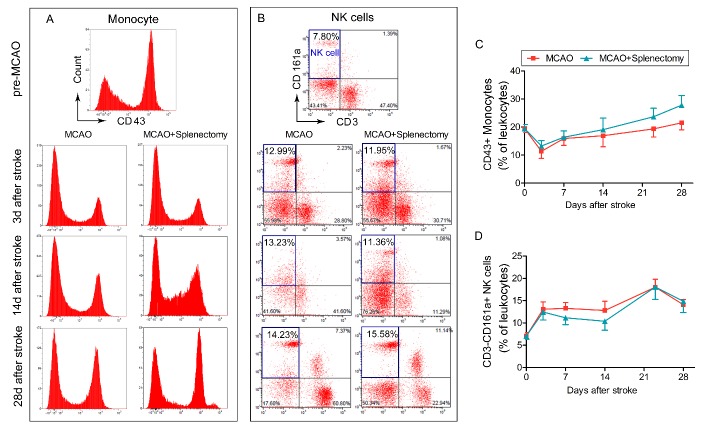
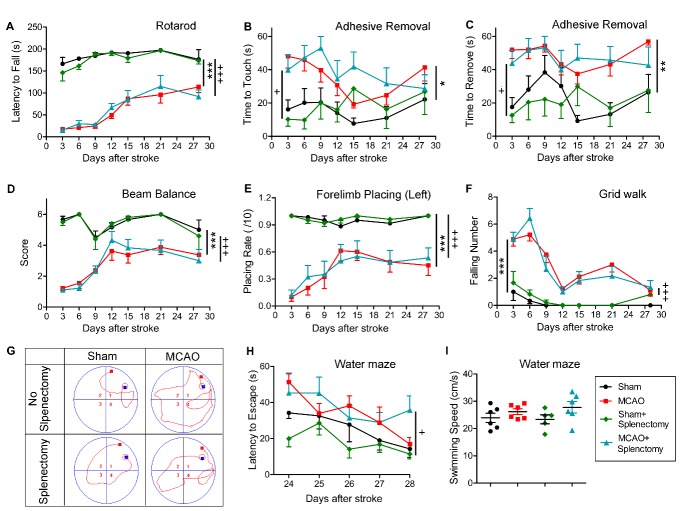
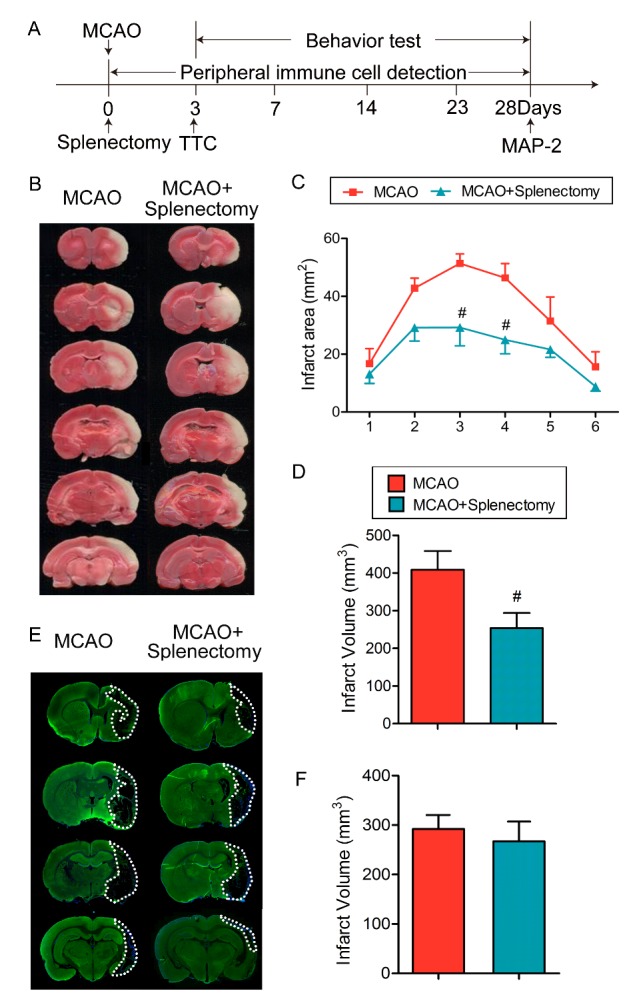
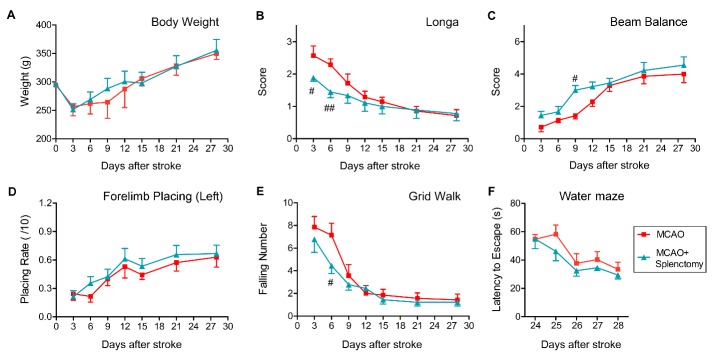
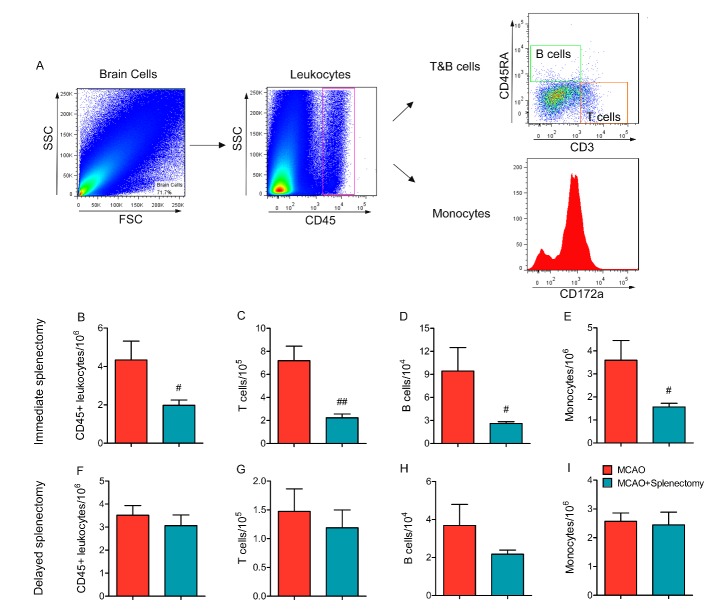
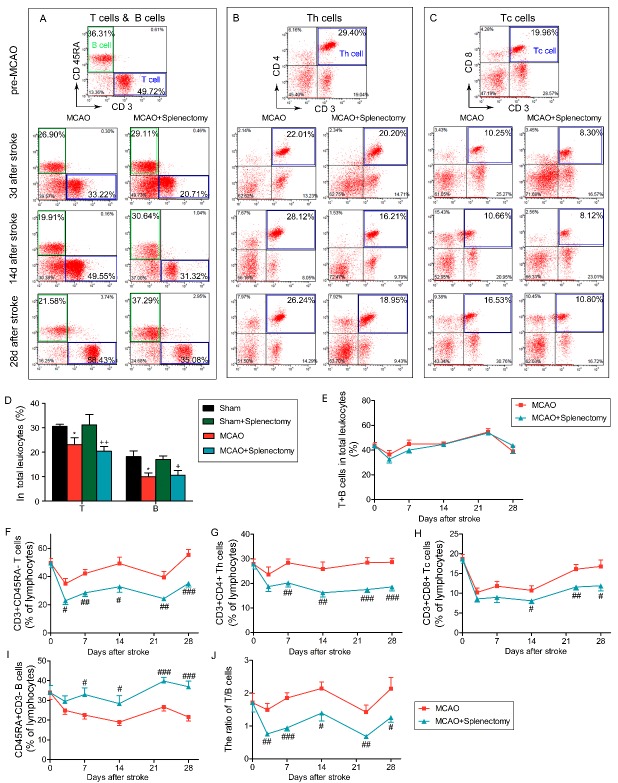
Splenectomy before or immediately after stroke provides early brain protection. This study aims to explore the effect of splenectomy on long-term neurological recovery after stroke, which is currently lacking in the field. Adult male rats were randomized into splenectomy or sham groups and then subjected to 90 min of middle cerebral artery occlusion (MCAO). Spleen was removed right upon reperfusion or 3d after MCAO. Infarct volume, neurological functions, and peripheral immune cell populations were assessed up to 28d after stroke. The results show that delayed removal of spleen did not reduce brain tissue loss and showed no effect on sensorimotor function (Rotarod, beam balance, forelimb placing, grid walk, and adhesive removal tests) or cognitive function (Morris water maze). Spleen removal immediately upon reperfusion, although significantly reduced the infarct size and immune cell infiltration 3d after MCAO, also failed to promote long-term recovery. Flow cytometry analysis demonstrated that immediate splenectomy after MCAO resulted in a prolonged decrease in the percentage of CD3CD4 and CD3CD8 T cells in total lymphocytes as compared to non-splenectomy MCAO rats. In contrast, the percentage of CD3CD45RA B cells was significantly elevated after splenectomy. As a result, the ratio of T/B cells was significantly reduced in stroke rats with splenectomy. In conclusion, delayed splenectomy failed to provide long-term protection to the ischemic brain or improve functional recovery. The acute neuroprotective effect achieved by early splenectomy after stroke cannot last for long term. This loss of neuroprotection might be related to the prolonged disturbance in the T cell to B cell ratio.
中风前或中风后立即进行脾切除术可提供早期脑保护。本研究旨在探讨脾切除术对中风后长期神经功能恢复的影响,而该领域目前尚缺乏相关研究。成年雄性大鼠被随机分为脾切除组或假手术组,然后进行90分钟的大脑中动脉闭塞(MCAO)。在再灌注时或MCAO后3天切除脾脏。在中风后长达28天的时间里评估梗死体积、神经功能和外周免疫细胞群。结果表明,延迟切除脾脏并未减少脑组织损失,对感觉运动功能(转棒试验、光束平衡试验、前肢放置试验、网格行走试验和粘胶去除试验)或认知功能(莫里斯水迷宫试验)也没有影响。再灌注时立即切除脾脏,虽然在MCAO后3天显著减小了梗死面积并减少了免疫细胞浸润,但也未能促进长期恢复。流式细胞术分析表明,与未进行脾切除的MCAO大鼠相比,MCAO后立即进行脾切除术导致总淋巴细胞中CD3CD4和CD3CD8 T细胞百分比持续下降。相反,脾切除术后CD3CD45RA B细胞百分比显著升高。因此,脾切除的中风大鼠中T/B细胞比值显著降低。总之,延迟脾切除术未能为缺血性脑提供长期保护或改善功能恢复。中风后早期脾切除术所实现的急性神经保护作用不能长期持续。这种神经保护作用的丧失可能与T细胞与B细胞比值的长期紊乱有关。