Tetreault Matthew W, Estrera Kenneth A, Kayupov Erdan, Brander Caroline, Della Valle Craig J
Department of Orthopaedic Surgery, Rush University Medical Center, Chicago, IL, USA.
Department of Orthopaedic Surgery, University of Texas Southwestern Medical Center, Dallas, TX, USA.
Arthroplast Today. 2017 Nov 10;4(2):216-220. doi: 10.1016/j.artd.2017.10.001. eCollection 2018 Jun.
Patients with a painful or failed total joint arthroplasties should be evaluated for periprosthetic joint infection (PJI). The purpose of this study is to determine if patients referred to a tertiary care center had been evaluated for PJI according to the American Academy of Orthopaedic Surgeons (AAOS) clinical practice guidelines.
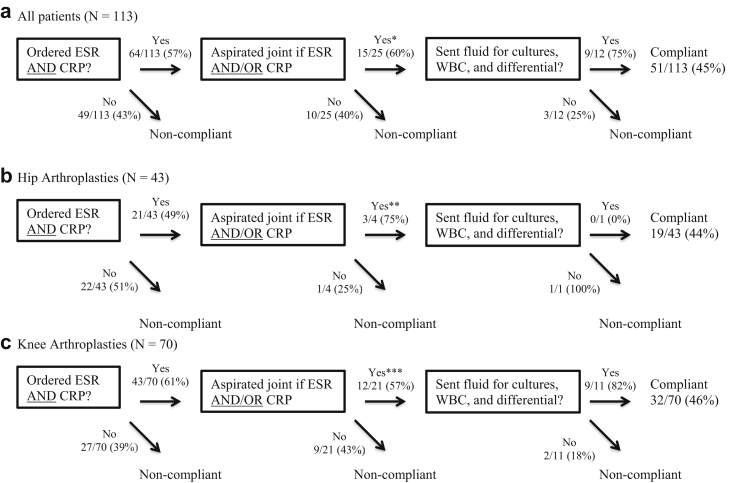
One hundred thirteen patients with painful hip (43) or knee (70) arthroplasties were referred to a single provider by orthopaedic surgeons outside our practice between 2012 and 2014. We retrospectively evaluated the workup by referring physicians, including measurement of serum erythrocyte sedimentation rate and C-reactive protein, performance of a joint aspiration if these values were abnormal, and obtainment of synovial fluid white blood cell count, differential, and cultures.
Sixty-two of 113 patients (55%) did not have a workup that followed AAOS guidelines. Serum erythrocyte sedimentation rate and C-reactive protein were ordered for 64 of the 113 patients (57%). Of 25 patients with elevated inflammatory markers warranting aspiration, 15 (60%) had an aspiration attempted, with synovial fluid white blood cell, differential, and cultures obtained in 9 of 12 (75%) aspirations that yielded fluid. Of the 62 patients with an incomplete infection workup, 11 (18%) had a bone scan, 6 (10%) a computed tomography scan, and 3 (5%) a magnetic resonance imaging. Twelve of the 113 patients (11%) were ultimately diagnosed with PJI, with 5 undiagnosed prior to referral.
The AAOS guidelines to evaluate for PJI are frequently not being followed. Improving awareness of these guidelines may avoid unnecessary and costly evaluations and delay in the diagnosis of PJI.
疼痛或失败的全关节置换患者应接受假体周围关节感染(PJI)评估。本研究的目的是确定转诊至三级医疗中心的患者是否根据美国矫形外科医师学会(AAOS)临床实践指南接受了PJI评估。
2012年至2014年间,113例髋部(43例)或膝部(70例)疼痛性关节置换患者由我们科室以外的骨科医生转诊至同一医疗服务提供者处。我们回顾性评估了转诊医生的检查过程,包括血清红细胞沉降率和C反应蛋白的测定,若这些值异常则进行关节穿刺,以及获取滑液白细胞计数、分类和培养结果。
113例患者中有62例(55%)未按照AAOS指南进行检查。113例患者中有64例(57%)进行了血清红细胞沉降率和C反应蛋白检查。在25例炎症指标升高需要穿刺的患者中,15例(60%)尝试进行了穿刺,12例穿刺成功获得液体的患者中有9例(75%)进行了滑液白细胞计数、分类和培养。在62例感染检查不完整的患者中,11例(18%)进行了骨扫描,6例(10%)进行了计算机断层扫描,3例(5%)进行了磁共振成像。113例患者中有12例(11%)最终被诊断为PJI,其中5例在转诊前未被诊断。
评估PJI的AAOS指南经常未被遵循。提高对这些指南的认识可能避免不必要且昂贵的检查以及PJI诊断的延迟。