Tan Nicole Lay Tin, Hunt Justin Lindley, Gwini Stella May
Honorary Clinical Fellow, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Melbourne, Australia.
Epworth HealthCare, 89 Bridge Rd, Richmond, Vic, 3121, Australia.
BMC Anesthesiol. 2018 Jun 13;18(1):64. doi: 10.1186/s12871-018-0525-5.
Enhanced recovery after surgery programs may improve recovery and reduce duration of hospital stay after joint replacement surgery. However, uptake is incomplete, and the relative importance of program components is unknown. This before-and-after quality improvement study was designed to determine whether adding 'non-surgical' components, to pre-existing 'surgical' components, in an Australian private healthcare setting, would improve patient recovery after total hip replacement.
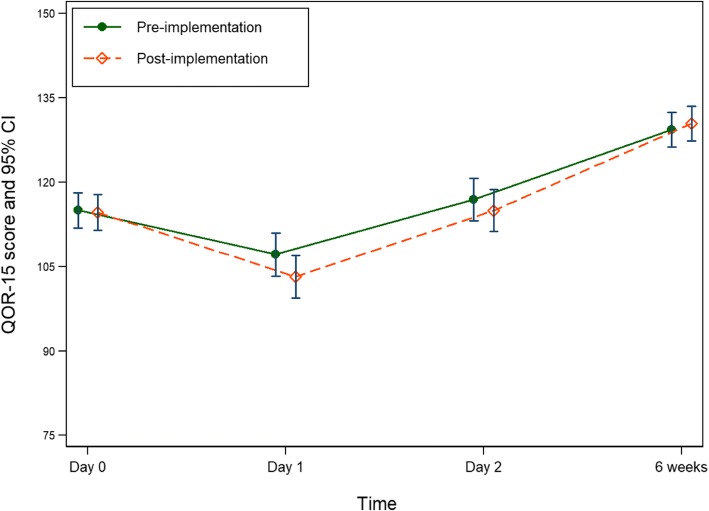
We prospectively collected data regarding care processes and health outcomes of 115 consecutive patients undergoing hip replacement with a single surgeon in a private hospital in Melbourne, Australia. Based on this data, a multidisciplinary team (surgeon, anesthetists, nurse unit managers, physiotherapists, perioperative physician) chose and implemented 12 'non-surgical' program components. Identical data were collected from a further 115 consecutive patients. The primary outcome measure was Quality of Recovery-15 score at 6 weeks postoperatively; the linear regression model was adjusted for baseline group differences.
The majority of health outcomes, including the primary outcome measure, were similar in pre- and post-implementation groups (quality of recovery score, pain rating and disability score, at time-points up to six weeks postoperatively). The proportion of patients with zero oral morphine equivalent consumption at six weeks increased from 57 to 80% (RR 1.34, 95% CI 1.13, 1.58). Mean (SD) length of hospital stay decreased from 5.94 (5.21) to 5.02 (2.46) days but was not statistically significant once adjusted for baseline group differences. Four of ten measurable program components were successfully implemented. Antiemetic prophylaxis increased by 53% (risk ratio [RR] 95% confidence interval [CI] 1.16, 2.02). Tranexamic acid use increased by 41% (RR 95% CI 1.18, 1.68). Postoperative physiotherapy treatment on the day of surgery increased by 87% (RR 95% CI 1.36, 2.59). Postoperative patient mobilisation ≥ three metres on the day of surgery increased by 151% (RR 95% CI 1.27, 4.97).
Implementation of a full enhanced recovery after surgery program, and optimal choice of program components, remains a challenge. Improved implementation of non-surgical components of a program may further reduce duration of acute hospital stay, while maintaining quality of recovery.
Australian New Zealand Clinical Trials Registry ( ACTRN12615001170516 ), 2.11.2015 (retrospective).
术后加速康复计划可能会改善关节置换手术后的恢复情况并缩短住院时间。然而,该计划的采用情况并不理想,且各组成部分的相对重要性尚不清楚。这项前后对照的质量改进研究旨在确定,在澳大利亚的私立医疗环境中,在现有的“手术”组成部分基础上增加“非手术”组成部分,是否会改善全髋关节置换术后患者的恢复情况。
我们前瞻性收集了澳大利亚墨尔本一家私立医院中,由同一位外科医生为115例连续接受髋关节置换手术患者提供的护理过程和健康结局数据。基于这些数据,一个多学科团队(外科医生、麻醉师、护士单元经理、物理治疗师、围手术期医生)选择并实施了12个“非手术”计划组成部分。又从另外115例连续患者中收集了相同的数据。主要结局指标是术后6周时的恢复质量-15评分;线性回归模型针对基线组差异进行了调整。
大多数健康结局,包括主要结局指标,在实施前后的组间相似(术后六周内各时间点的恢复质量评分、疼痛评分和残疾评分)。术后六周口服吗啡当量消耗量为零的患者比例从57%增至80%(相对危险度1.34,95%置信区间1.13,1.58)。平均(标准差)住院时间从5.94(5.21)天降至5.02(2.46)天,但在针对基线组差异进行调整后无统计学意义。十个可衡量的计划组成部分中有四个成功实施。预防性使用止吐药增加了53%(风险比[RR]95%置信区间[CI]1.16,2.02)。氨甲环酸的使用增加了41%(RR 95% CI 1.18,1.68)。术后第一天进行物理治疗的患者增加了87%(RR 95% CI 1.36,2.59)。术后第一天患者活动距离≥三米的情况增加了151%(RR 95% CI 1.27,4.97)。
全面实施术后加速康复计划以及对计划组成部分进行最佳选择仍然是一项挑战。更好地实施计划中的非手术组成部分可能会进一步缩短急性住院时间,同时保持恢复质量。
澳大利亚和新西兰临床试验注册中心(ACTRN12615001170516),2015年11月2日(回顾性)