Wilson Alastair, Bath Philip Mw, Berge Eivind, Cadilhac Dominique A, Cuche Matthieu, Ford Gary A, Macisaac Rachael, Quinn Terence J, Taylor Matthew, Walters Matthew, Wolff Claudia, Lees Kennedy R
Institute of Cardiovascular and Medical Sciences, University of Glasgow, Queen Elizabeth University Hospital, Glasgow, UK.
Stroke Trials Unit, Division of Clinical Neuroscience, University of Nottingham, City Hospital Campus, Nottingham, UK.
Eur Stroke J. 2017 Mar;2(1):3-12. doi: 10.1177/2396987316684705. Epub 2016 Dec 22.
Cost-of-illness studies often describe a single aggregate cost of a disease state. This approach is less helpful for a condition with a spectrum of outcomes like stroke. The modified Rankin Scale is the most commonly used outcome measure for stroke. We sought to describe the existing evidence on the costs of stroke according to individual modified Rankin Scale categories. This may be useful in future cost effectiveness modelling studies of interventions where cost data have not been collected, but disability outcome is known.
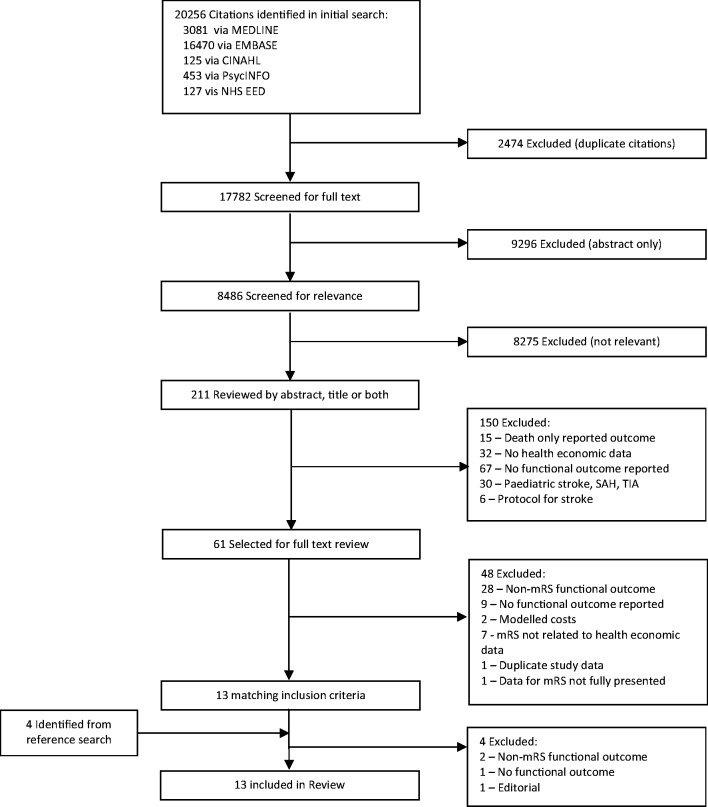
Systematic review of the published literature, searching electronic databases between 2004 and 2015 using validated search filters. Results were screened to identify studies presenting costs by individual modified Rankin Scale categories.
Of 17,782 unique identified articles, 13 matched all inclusion criteria. In only four of these studies were costs reported by modified Rankin Scale categories. Most studies included direct medical costs only. Societal costs were assessed in two studies. Overall, studies had a high methodological and reporting quality. The heterogeneity in costing methods used in the identified studies prevented meaningful comparison of the reported cost data. Despite this limitation, the costs consistently increased with greater severity (increasing modified Rankin Scale score).
Few cost studies of stroke include information based on stroke recovery measured by individual modified Rankin Scale categories and the existing data are limited. To reliably capture this information, future studies are needed that preferably apply standardised costing methods to promote greater potential for use in cost-effectiveness analyses whereby direct collection of patient-level resource use has not been possible.
疾病成本研究通常描述疾病状态的单一总成本。这种方法对于像中风这样具有一系列不同结局的疾病帮助较小。改良Rankin量表是中风最常用的结局指标。我们试图根据改良Rankin量表的各个类别来描述中风成本的现有证据。这对于未来在尚未收集成本数据但已知残疾结局的干预措施成本效益建模研究中可能有用。
对已发表文献进行系统综述,使用经过验证的检索过滤器在2004年至2015年期间检索电子数据库。对结果进行筛选,以识别按改良Rankin量表各个类别呈现成本的研究。
在17782篇唯一识别的文章中,有13篇符合所有纳入标准。其中只有4项研究按改良Rankin量表类别报告了成本。大多数研究仅包括直接医疗成本。两项研究评估了社会成本。总体而言,研究具有较高的方法学和报告质量。已识别研究中使用的成本核算方法的异质性妨碍了对报告成本数据进行有意义的比较。尽管有此限制,但成本随着严重程度增加(改良Rankin量表得分增加)而持续上升。
很少有中风成本研究包含基于改良Rankin量表各个类别测量的中风恢复情况的信息,现有数据有限。为了可靠地获取这些信息,未来需要开展研究,最好采用标准化成本核算方法,以提高在成本效益分析中的应用潜力,因为直接收集患者层面的资源使用情况是不可能的。