Departments of Pathology and Laboratory Medicine (M.K., S.L.) Community Health Sciences (L.S.C.), University of Calgary Department of Cancer Epidemiology and Prevention Research, Alberta Health Services-Cancer Control Alberta (X.G., L.S.C.), Calgary, Alberta Canada's Michael Smith Genome Sciences Centre, BC Cancer Agency, Vancouver; and Department of Biomedical Physiology and Kinesiology, Simon Fraser University, Burnaby (A.B.-W.) Department of Pathology and Laboratory Medicine, University of British Columbia (C.B.G.) Cancer Control Research, BC Cancer Research Centre (N.D.L.), Vancouver, British Columbia, Canada Department of Internal Medicine, Division of Epidemiology, Biostatistics and Preventive Medicine, UNM Comprehensive Cancer Center, University of New Mexico, Albuquerque, New Mexico (L.L., L.S.C.).
Int J Gynecol Pathol. 2019 Jul;38(4):353-362. doi: 10.1097/PGP.0000000000000530.
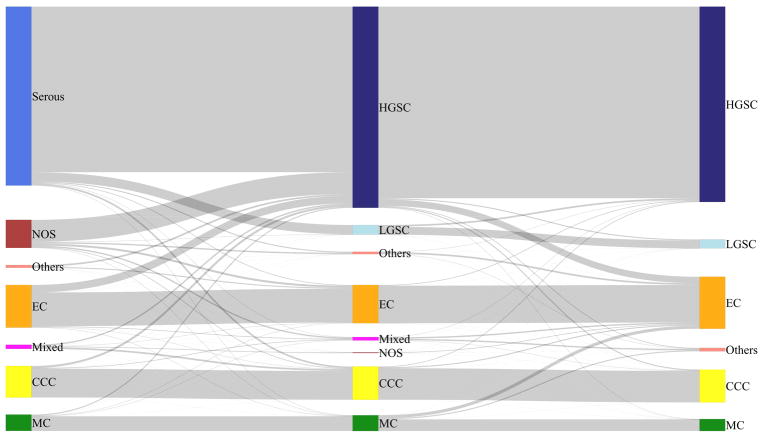
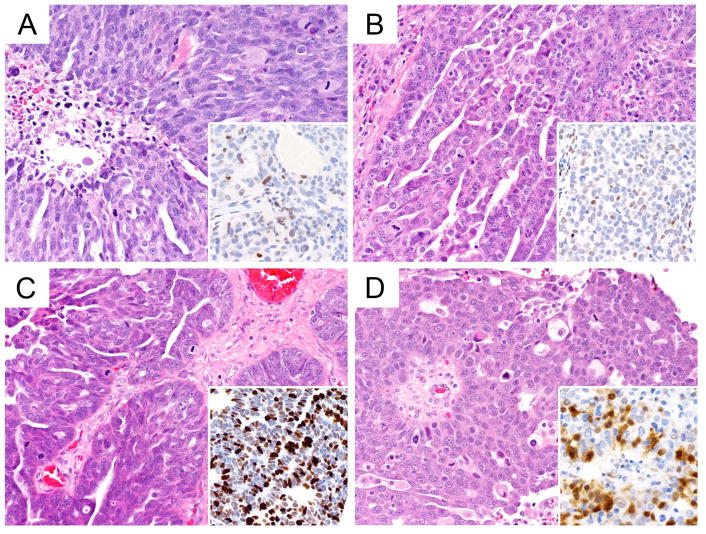
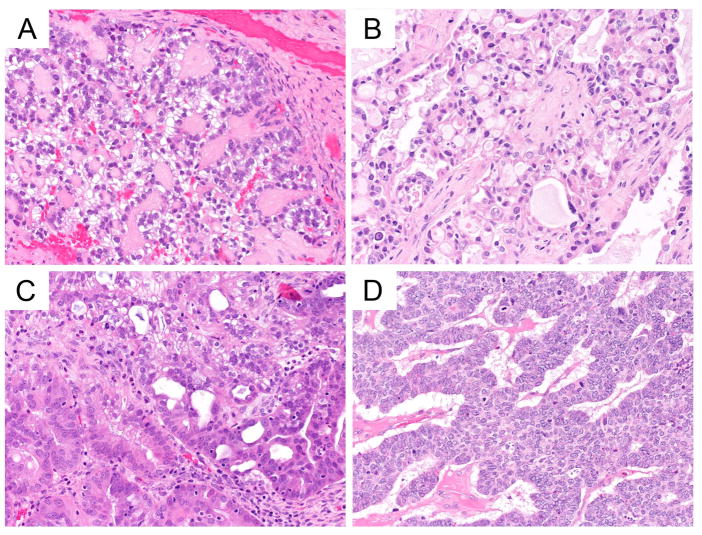
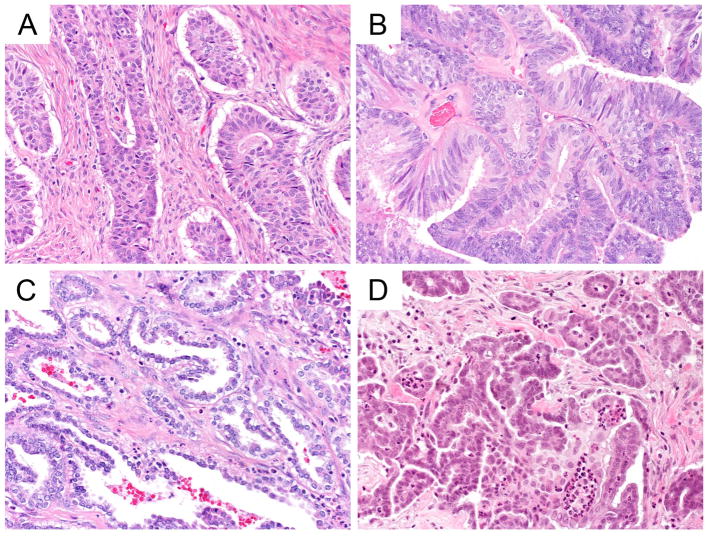
Ovarian carcinoma histotypes are critical for research and patient management and currently assigned by a combination of histomorphology +/- ancillary immunohistochemistry (IHC). We aimed to validate the previously described IHC algorithm (Calculator of Ovarian carcinoma Subtype/histotype Probability version 3, COSPv3) in an independent population-based cohort, and to identify problem areas for IHC predictions. Histotype was abstracted from cancer registries for eligible ovarian carcinoma cases diagnosed from 2002 to 2011 in Alberta and British Columbia, Canada. Slides were reviewed according to World Health Organization 2014 criteria, tissue microarrays were stained with and scored for the 8 COSPv3 IHC markers, and COSPv3 histotype predictions were calculated. Discordant cases for review and COSPv3 prediction were arbitrated by integrating morphology with IHC results. The integrated histotype (N=880) was then used to identify areas of inferior COSPv3 performance. Review histotype and integrated histotype demonstrated 93% agreement suggesting that IHC information revises expert review in up to 7% of cases. There was also 93% agreement between COSPv3 prediction and integrated histotype. COSPv3 errors predominated in 4 areas: endometrioid carcinoma (EC) versus clear cell (N=23), EC versus low-grade serous (N=15), EC versus high-grade serous (N=11), and high-grade versus low-grade serous (N=6). Most problems were related to Napsin A-negative clear cell, WT1-positive EC, and p53 IHC wild-type high-grade serous carcinomas. Although 93% of COSPv3 prediction accuracy was validated, some histotyping required integration of morphology with ancillary test results. Awareness of these limitations will avoid overreliance on IHC and misclassification of histotypes for research and clinical management.
卵巢癌组织学类型对研究和患者管理至关重要,目前主要通过组织形态学+/-辅助免疫组织化学(IHC)来确定。我们旨在验证先前描述的 IHC 算法(卵巢癌亚型/组织学分型概率计算器第 3 版,COSPv3)在一个独立的基于人群的队列中的有效性,并确定 IHC 预测的问题领域。从加拿大艾伯塔省和不列颠哥伦比亚省 2002 年至 2011 年诊断的合格卵巢癌病例的癌症登记处中提取组织学类型。根据 2014 年世界卫生组织标准对切片进行审查,使用 8 种 COSPv3 IHC 标志物对组织微阵列进行染色和评分,并计算 COSPv3 组织学类型预测。对有争议的病例进行审查和 COSPv3 预测,通过整合形态学和 IHC 结果进行仲裁。然后,使用整合的组织学类型(N=880)来确定 COSPv3 性能较差的区域。审查组织学类型和整合组织学类型之间的一致性为 93%,这表明 IHC 信息在多达 7%的病例中修正了专家审查。COSPv3 预测和整合组织学类型之间也有 93%的一致性。COSPv3 错误主要集中在 4 个方面:子宫内膜样癌(EC)与透明细胞癌(N=23)、EC 与低级别浆液性癌(N=15)、EC 与高级别浆液性癌(N=11)和高级别与低级别浆液性癌(N=6)。大多数问题与 Napsin A 阴性透明细胞癌、WT1 阳性 EC 和 p53 IHC 野生型高级别浆液性癌有关。尽管 COSPv3 预测准确率为 93%,但某些组织学类型需要整合形态学和辅助测试结果。了解这些局限性将避免过度依赖 IHC 和对研究和临床管理的组织学分型的错误分类。