Clinica Valle Giulia, G.EN.E.R.A. Centers for Reproductive Medicine, Rome, Italy.
Clinica Ruesch, G.EN.E.R.A. Centers for Reproductive Medicine, Naples, Italy.
Hum Reprod. 2018 Aug 1;33(8):1442-1448. doi: 10.1093/humrep/dey217.
Are the mean numbers of blastocysts obtained from sibling cohorts of oocytes recruited after follicular phase and luteal phase stimulations (FPS and LPS) in the same ovarian cycle similar?
The cohorts of oocytes obtained after LPS are larger than their paired-FPS-derived cohorts and show a comparable competence, thus resulting in a larger mean number of blastocysts.
Three theories of follicle recruitment have been postulated to date: (i) the 'continuous recruitment' theory, (ii) the 'single recruitment episode' theory and (iii) the 'wave' theory. Yet, a clear characterization of this crucial biological process for human reproduction is missing. Recent advances implemented in in vitro fertilization (IVF), such as blastocyst culture, aneuploidy testing and vitrification, have encouraged clinicians to maximize the exploitation of the ovarian reserve through tailored stimulation protocols, which is crucial especially for poor prognosis patients aiming to conceive after IVF. LPS has been already successfully adopted to treat poor prognosis or oncological patients through Duostim, LPS-only or random-start ovarian stimulation approaches. Nevertheless, little, and mainly retrospective, evidence has been produced to support the safety of LPS in general. Feasibility of the LPS approach would severely question the classic 'single recruitment episode' theory of follicular development.
STUDY DESIGN, SIZE, DURATION: This case-control study was conducted with paired follicular phase- and luteal phase-derived cohorts of oocytes collected after stimulations in the same ovarian cycle (DuoStim) at two private IVF clinics between October 2015 and December 2017.
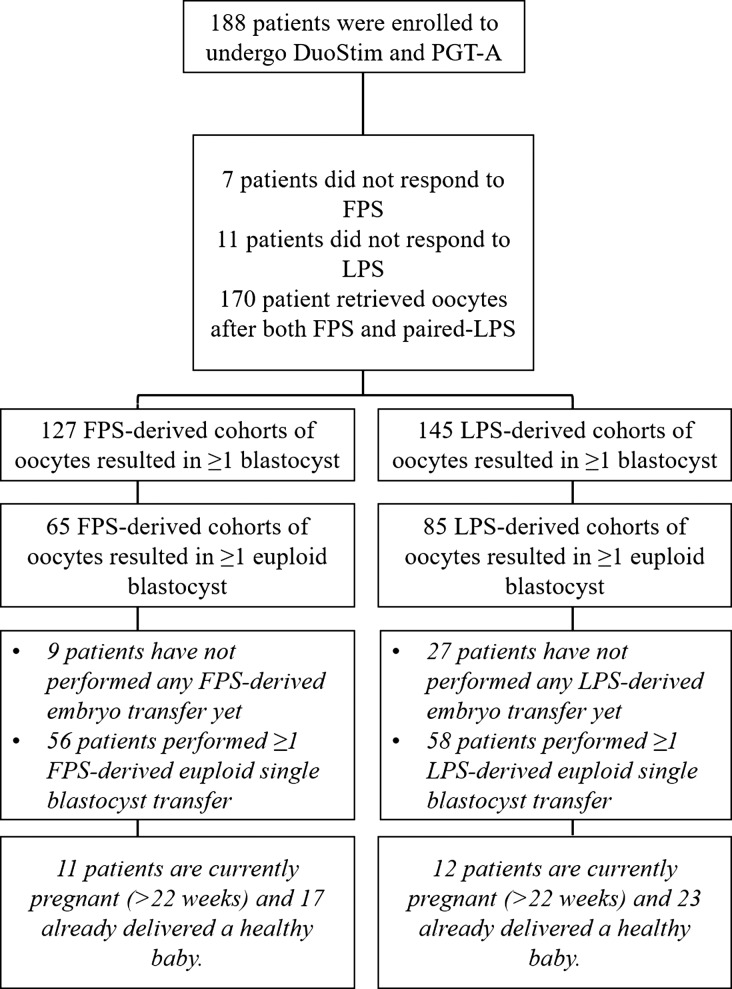
PARTICIPANTS/MATERIALS, SETTING, METHODS: The study included 188 poor prognosis patients undergoing DuoStim with preimplantation genetic testing for aneuploidies (PGT-A). FPS and LPS were performed with the same daily dose of recombinant-gonadotrophins in an antagonist protocol. Blastocyst culture, trophectoderm biopsy, vitrification and frozen-warmed euploid single blastocyst transfers were performed. The primary outcome was the mean number of blastocysts obtained per oocyte retrieval from paired-FPS- and LPS-derived cohorts (required sample size = 165 patients; power = 90%). Mean blastulation and euploidy rates were monitored, along with the number of oocytes, euploid blastocysts and clinical outcomes.
Significantly fewer blastocysts were obtained after FPS than LPS (1.2 ± 1.1 vs. 1.6 ± 1.6, P < 0.01), due to fewer oocytes collected (3.6 ± 2.1 vs. 4.3 ± 2.8, P < 0.01) and a similar mean blastocyst rates per retrieval (33.1% ± 30.3% vs. 37.4% ± 30.8%, P = NS). The number of oocytes collected were correlated (R = 0.5, P < 0.01), while the blastocyst rates were uncorrelated among paired-FPS- and LPS-derived cohorts. Overall, a significantly lower chance of producing blastocyst(s) was reported after FPS than after LPS: 67.6% (n = 127/188, 95%CI: 60.3-74.1) vs. 77.1% (n = 145/188, 95%CI: 70.3-82.8; P = 0.05). The mean euploidy rates per retrieval were similar between FPS- and LPS-derived cohorts of oocytes (13.6% ± 22.8% vs. 16.3% ± 23.4%, P = NS). Therefore, on average fewer euploid blastocysts (0.5 ± 0.8 vs. 0.7 ± 1.0, P = 0.02) resulted from FPS. Similar ongoing-pregnancy/delivery rates were reported, to date, after FPS- and LPS-derived euploid single blastocyst transfers: 42.4% (n = 28/66, 95%CI: 30.5-55.2) vs. 53.8% (n = 35/65, 95%CI: 41.1-66.1; P = NS).
LIMITATIONS, REASONS FOR CAUTION: More studies need to be conducted in the future to confirm the safety of LPS, especially in terms of ovarian and follicular environment, as well as the clinical, peri-natal and post-natal outcomes. Here, we showed preliminary data suggesting a similar ongoing implantation/delivery rate (>22 weeks) between FPS- and LPS-derived euploid blastocysts, that need to be extended in the future, to populations other than poor prognosis patients and using approaches other than DuoStim together with a constant monitoring of the related peri-natal and post-natal outcomes.
These data, from a paired study design, highlight that LPS-derived oocytes are as competent as FPS-derived oocytes, thereby adding some evidence to support the use of LPS for poor prognosis and oncological patients and to question the 'single recruitment episode' theory of follicle recruitment. These findings also encourage additional studies of the basics of folliculogenesis, with direct clinical implications for the management of ovarian stimulation in IVF.
None.
STUDY FUNDING/COMPETING INTEREST(S): No external funds were used for this study and there are no conflicts of interest.
在同一个卵巢周期中,从卵泡期和黄体期刺激(FPS 和 LPS)募集的同胞卵母细胞队列获得的胚泡平均数是否相似?
与配对的 FPS 衍生队列相比,LPS 获得的卵母细胞数量更大,且具有相当的能力,因此导致胚泡平均数更大。
迄今为止,已经提出了三种卵泡募集理论:(i)“连续募集”理论,(ii)“单次募集事件”理论和(iii)“波”理论。然而,对于人类生殖的这一关键生物学过程,仍然缺乏明确的描述。最近在体外受精(IVF)中实施的一些进展,如胚泡培养、非整倍体检测和玻璃化,鼓励临床医生通过量身定制的刺激方案来最大限度地利用卵巢储备,这对于希望在 IVF 后怀孕的预后不良或肿瘤患者尤为重要。LPS 已通过 Duostim、LPS 仅或随机启动卵巢刺激方法成功用于治疗预后不良或肿瘤患者。然而,目前只有少量且主要是回顾性的证据支持 LPS 一般情况下的安全性。LPS 方法的可行性将严重质疑经典的卵泡发育“单次募集事件”理论。
研究设计、规模、持续时间:本病例对照研究采用配对的卵泡期和黄体期衍生的卵母细胞队列,这些卵母细胞是在 2015 年 10 月至 2017 年 12 月在两家私人 IVF 诊所进行的同一卵巢周期中的刺激(DuoStim)中收集的。
参与者/材料、地点、方法:该研究纳入了 188 名接受预植入遗传检测以排除非整倍体(PGT-A)的预后不良患者。FPS 和 LPS 均在拮抗剂方案中以相同的每日重组促性腺激素剂量进行。进行胚泡培养、滋养外胚层活检、玻璃化和冷冻解冻后的整倍体单囊胚转移。主要结局是从配对的 FPS 和 LPS 衍生的卵母细胞队列中获得的每个卵母细胞的平均胚泡数(所需样本量=165 例;功率=90%)。监测了平均胚泡化率和整倍体率,以及卵母细胞数量、整倍体胚泡数量和临床结局。
与 LPS 相比,FPS 后获得的胚泡数量明显较少(1.2±1.1 比 1.6±1.6,P<0.01),这是由于收集的卵母细胞较少(3.6±2.1 比 4.3±2.8,P<0.01)和相似的平均每个取卵的胚泡率(33.1%±30.3%比 37.4%±30.8%,P=NS)。收集的卵母细胞数量相关(R=0.5,P<0.01),而 FPS 和 LPS 衍生的卵母细胞队列之间的胚泡率不相关。总体而言,与 LPS 相比,FPS 后产生胚泡的机会明显较低:67.6%(n=127/188,95%CI:60.3-74.1)比 77.1%(n=145/188,95%CI:70.3-82.8;P=0.05)。FPS 和 LPS 衍生的卵母细胞队列的平均整倍体率相似(13.6%±22.8%比 16.3%±23.4%,P=NS)。因此,平均而言,FPS 产生的整倍体胚泡数量较少(0.5±0.8 比 0.7±1.0,P=0.02)。迄今为止,在 FPS 和 LPS 衍生的整倍体单囊胚转移后,报告了相似的持续妊娠/分娩率:42.4%(n=28/66,95%CI:30.5-55.2)比 53.8%(n=35/65,95%CI:41.1-66.1;P=NS)。
局限性、谨慎的原因:未来需要进行更多的研究来确认 LPS 的安全性,特别是在卵巢和卵泡环境以及临床、围产期和产后结局方面。在这里,我们展示了初步数据,表明 FPS 和 LPS 衍生的整倍体胚泡具有相似的持续着床/分娩率(>22 周),这需要在未来扩展到预后不良的患者群体以外,并使用 DuoStim 以外的其他方法,同时持续监测相关的围产期和产后结局。
这些来自配对研究设计的数据强调,LPS 衍生的卵母细胞与 FPS 衍生的卵母细胞一样具有能力,从而为使用 LPS 治疗预后不良和肿瘤患者提供了一些证据,并对“单次募集事件”理论提出了质疑。这些发现还鼓励对卵泡发生的基础进行进一步研究,对 IVF 中卵巢刺激的管理具有直接的临床意义。
无。
研究资金/利益冲突:本研究没有外部资金,也没有利益冲突。