Kaballo Mohammed A, Canney Mark, O'Kelly Patrick, Williams Yvonne, O'Seaghdha Conall M, Conlon Peter J
Department of Nephrology and Transplantation, Beaumont Hospital, Dublin, Ireland.
Clin Kidney J. 2018 Jun;11(3):389-393. doi: 10.1093/ckj/sfx117. Epub 2017 Oct 18.
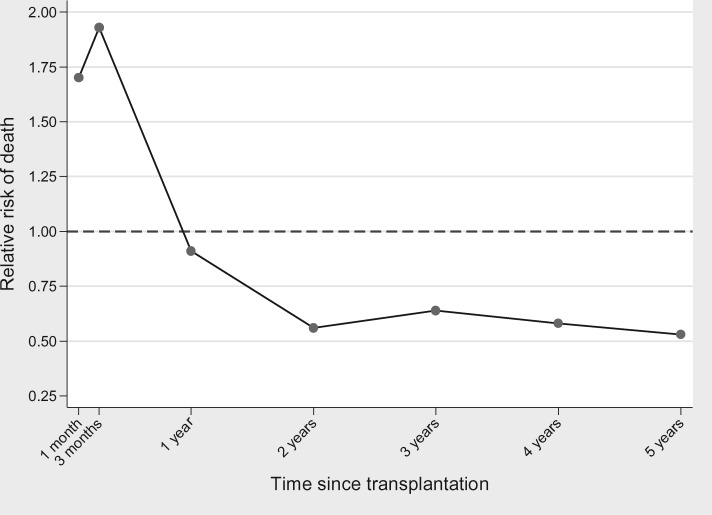
Kidney transplant survival benefits are not observed for around 8 months after transplantation because of a higher complications rate in early post-transplant periods. This study compares survival of patients awaiting transplantation with survival of transplant recipients and non-listed dialysis patients in Ireland.
In this retrospective analysis, the relative-risk (RR) of death was assessed with time-dependent, non-proportional hazards analysis, with adjustment for age, cause of end-stage kidney disease (ESKD), time from first treatment for ESKD to placement on the waiting list and year of initial placement on the list.
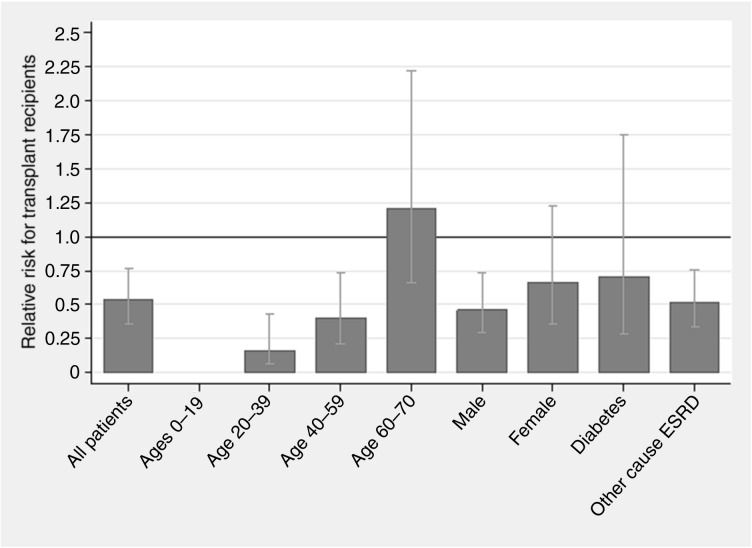
A total of 3597 patients were included. Annual death rates per 100 patient-years at risk for all patients on dialysis, waiting-list patients and transplant recipients were 16.5, 2.4 and 1.2, respectively. Death rate was highest among diabetics. The relative risk of death for all patients on dialysis was five times higher than the waiting-list patients [RR, 4.90; 95% confidence interval (CI), 3.70-6.52; P < 0.001]. Time to survival equilibration was 1 year. Thereafter, the 5-year mortality risk was estimated to be 47% lower than that of the patients on the waiting list (RR, 0.53; 95% CI, 0.37-0.77; P = 0.001).
Transplant recipients had a higher risk of death initially, but a better long-term survival. Time to death risk equilibration was longer compared with other studies. This could be explained by better survival rates in our waiting-list cohort.
由于移植后早期并发症发生率较高,肾移植患者在移植后约8个月内未观察到生存获益。本研究比较了爱尔兰等待移植患者、移植受者和未列入名单的透析患者的生存率。
在这项回顾性分析中,采用时间依赖性非比例风险分析评估死亡相对风险,并对年龄、终末期肾病(ESKD)病因、从首次治疗ESKD到列入等待名单的时间以及首次列入名单的年份进行调整。
共纳入3597例患者。所有透析患者、等待名单患者和移植受者每100患者年的年死亡率分别为16.5、2.4和1.2。糖尿病患者的死亡率最高。所有透析患者的死亡相对风险比等待名单患者高五倍[相对风险(RR),4.90;95%置信区间(CI),3.70 - 6.52;P < 0.001]。生存平衡时间为1年。此后,估计5年死亡风险比等待名单上的患者低47%(RR,0.53;95% CI,0.37 - 0.77;P = 0.001)。
移植受者最初死亡风险较高,但长期生存率较好。与其他研究相比,死亡风险平衡时间更长。这可能是由于我们等待名单队列中的生存率更高。