Auerbach Hematology and Oncology, Baltimore, MD, USA.
Georgetown University, Washington DC, USA.
Reprod Health. 2018 Jun 22;15(Suppl 1):96. doi: 10.1186/s12978-018-0536-1.
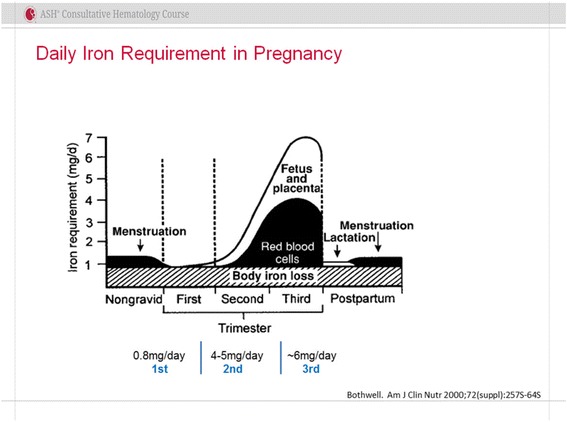
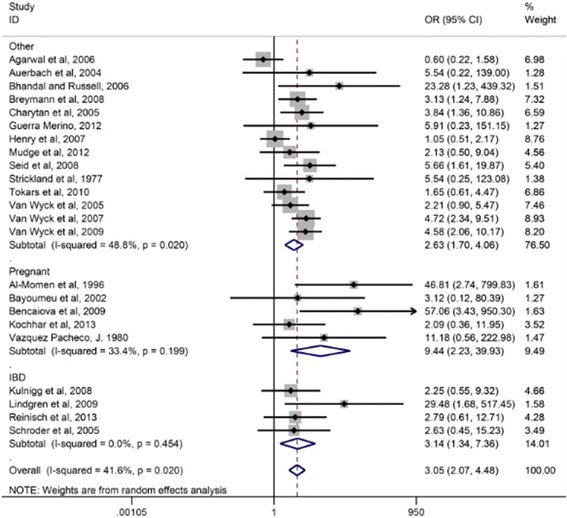
Iron deficiency anemia of pregnancy is common, especially in South Asia, and is associated with adverse maternal and fetal outcomes including increased incidences of maternal mortality, preterm labor and low birth weight. Screening for anemia alone is not sufficient to diagnose iron deficiency. Iron deficiency in neonates is associated with a statistically significant increment in cognitive and behavioral abnormalities which persist after iron repletion. Oral iron is the frontline standard but is associated with an unacceptably high incidence of gastrointestinal adverse events leading to poor adherence. Prospective evidence reports an incidence of neonatal iron deficiency up to 45% even with oral iron supplementation. New evidence reports oral iron ingestion increases serum hepcidin leading to decreased absorption suggesting further decreasing efficacy. Published evidence reports that intravenous iron is safe and effective in the second and third trimesters of pregnancy. Intravenous iron is the preferred route when there is oral iron intolerance or in those situations where oral iron is ineffective or harmful. Intravenous iron is also preferred if the anemia is severe (< 8 g/dL) in the second trimester or at any time in the third trimester when there is little expectation that adequate quantities of iron will be delivered to the fetus as iron requirements increase in each trimester. Guidelines for maternal and neonatal screening and treatment lack consistency and differ between the United States and Europe. New formulations of intravenous iron with complex carbohydrate cores that bind elemental iron more tightly mitigating the release of large quantities of labile free iron allow the administration of complete replacement doses in 15-60 min. The preponderance of published evidence suggests that intravenous iron is underutilized in pregnancy and guidelines suggesting there is insufficient evidence to recommend the routine screening and treatment of iron deficiency in gravidas should be revisited. The major recommendation from this commentary is that in low-income countries, a trial or demonstration project to test the efficacy, safety, cost and feasibility of the administration of intravenous iron to anemic and/or iron-deficient women be undertaken.
妊娠缺铁性贫血很常见,尤其是在南亚地区,与不良的母婴结局相关,包括增加孕产妇死亡率、早产和低出生体重。单独筛查贫血不足以诊断缺铁。新生儿缺铁与认知和行为异常的发生率显著增加相关,这些异常在补铁后仍持续存在。口服铁剂是一线标准治疗方法,但与之相关的胃肠道不良反应发生率高,导致患者顺应性差。前瞻性证据报告称,即使给予口服铁剂补充,新生儿缺铁的发生率仍高达 45%。新证据表明,口服铁剂摄入会导致血清铁调素增加,从而降低铁的吸收,这表明其疗效进一步降低。已发表的证据表明,静脉铁剂在妊娠第二和第三孕期是安全有效的。当存在口服铁不耐受,或口服铁无效或有害,或贫血在妊娠中期严重(<8g/dL)或在妊娠晚期任何时间时,首选静脉铁剂治疗。妊娠中、晚期铁需求每增加一个孕期时,指南都建议当贫血严重(<8g/dL)或任何时间在妊娠晚期时,当预期胎儿无法获得足够的铁时,选择静脉铁剂治疗。美国和欧洲的母婴筛查和治疗指南缺乏一致性,存在差异。新型静脉铁剂配方具有更紧密结合元素铁的复合碳水化合物核心,可减少大量不稳定游离铁的释放,允许在 15-60 分钟内给予全量替代剂量。已发表证据的主要观点表明,静脉铁剂在妊娠中未得到充分利用,应重新审视指南建议,即认为没有足够证据常规筛查和治疗孕妇缺铁的观点。本评论的主要建议是,在低收入国家,开展一项试验或示范项目,以测试静脉铁剂在贫血和/或缺铁孕妇中的疗效、安全性、成本和可行性。