Claridge Simon, Briceno Natalia, Chen Zhong, De Silva Kalpa, Modi Bhavik, Jackson Tom, Behar Jonathan M, Niederer Steven, Rinaldi Christopher A, Perera Divaka
Department of Imaging Sciences, King's College, London, United Kingdom.
NIHR Biomedical Research Centre, School of Cardiovascular Medicine and Sciences, King's College London, United Kingdom.
Int J Cardiol Heart Vasc. 2018 Apr 4;19:8-13. doi: 10.1016/j.ijcha.2018.03.002. eCollection 2018 Jun.
Biventricular pacing has been shown to increase both cardiac contractility and coronary flow acutely but the causal relationship is unclear. We hypothesised that changes in coronary flow are secondary to changes in cardiac contractility. We sought to examine this relationship by modulating coronary flow and cardiac contractility.
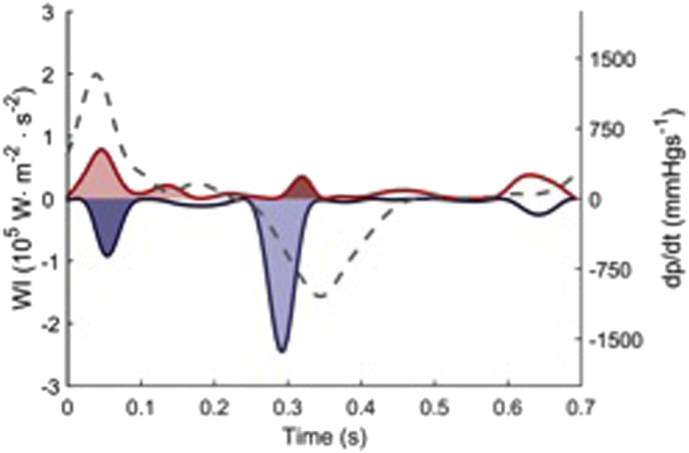
Contractility and lusitropy were altered by varying the location of pacing in 8 patients. Coronary autoregulation was transiently disabled with intracoronary adenosine. Simultaneous coronary flow velocity, coronary pressure and left ventricular pressure data were measured in the different pacing settings with and without hyperaemia and wave intensity analysis performed.
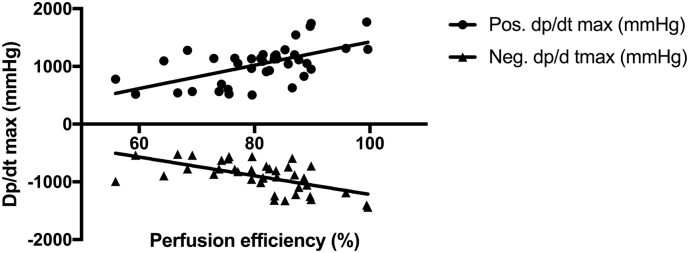
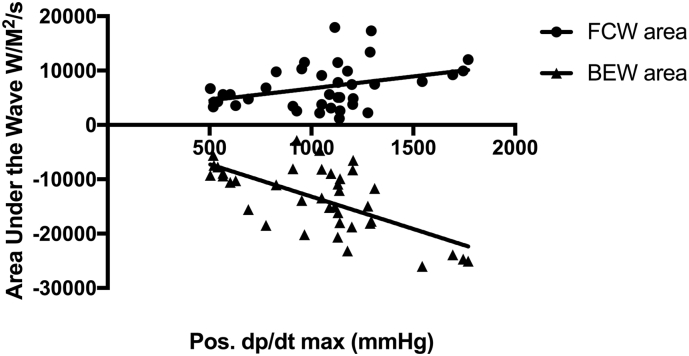
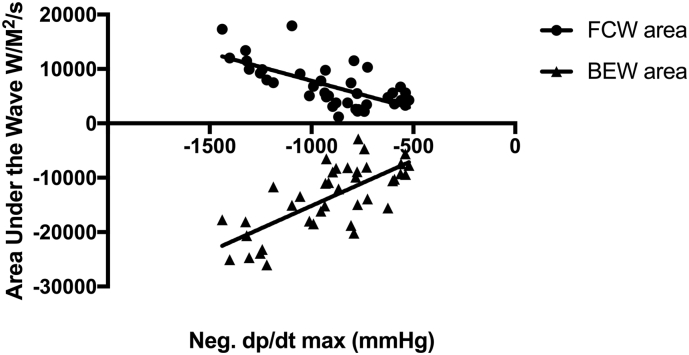
Multisite pacing was effective at altering left ventricular contractility and lusitropy (pos. dp/dt -13% to +10% and neg. dp/dt -15% to +17% compared to baseline). Intracoronary adenosine decreased microvascular resistance (362.5 mm Hg/s/m to 156.7 mm Hg/s/m, p < 0.001) and increased LAD flow velocity (22 cm/s vs 45 cm/s, p < 0.001) but did not acutely change contractility or lusitropy. The magnitude of the dominant accelerating wave, the Backward Expansion Wave, was proportional to the degree of contractility as well as lusitropy (r = 0.47, p < 0.01 and r = -0.50, p < 0.01). Perfusion efficiency (the proportion of accelerating waves) increased at hyperaemia (76% rest vs 81% hyperaemia, p = 0.04). Perfusion efficiency correlated with contractility and lusitropy at rest (r = 0.43 & -0.50 respectively, p = 0.01) and hyperaemia (r = 0.59 & -0.6, p < 0.01).
Acutely increasing coronary flow with adenosine in patients with systolic heart failure does not increase contractility. Changes in coronary flow with biventricular pacing are likely to be a consequence of enhanced cardiac contractility from resynchronization and not vice versa.
双心室起搏已被证明可急性增加心脏收缩力和冠状动脉血流量,但因果关系尚不清楚。我们假设冠状动脉血流量的变化继发于心脏收缩力的变化。我们试图通过调节冠状动脉血流量和心脏收缩力来研究这种关系。
通过改变8例患者的起搏位置来改变收缩力和舒张功能。冠状动脉自动调节通过冠状动脉内注射腺苷暂时失效。在有或无充血的不同起搏设置下测量冠状动脉血流速度、冠状动脉压力和左心室压力数据,并进行波强度分析。
多部位起搏有效地改变了左心室收缩力和舒张功能(与基线相比,正dp/dt为-13%至+10%,负dp/dt为-15%至+17%)。冠状动脉内注射腺苷降低了微血管阻力(从362.5mmHg/s/m降至156.7mmHg/s/m,p<0.001),增加了左前降支血流速度(从22cm/s增至45cm/s,p<0.001),但未急性改变收缩力或舒张功能。主导加速波,即向后扩展波的大小与收缩力和舒张功能的程度成正比(r=0.47,p<0.01和r=-0.50,p<0.01)。充血时灌注效率(加速波的比例)增加(静息时为76%,充血时为81%,p=0.04)。静息时灌注效率与收缩力和舒张功能相关(r分别为0.43和-0.50,p=0.01),充血时也相关(r为0.59和-0.6,p<0.01)。
在收缩性心力衰竭患者中,用腺苷急性增加冠状动脉血流量并不会增加收缩力。双心室起搏时冠状动脉血流量的变化可能是再同步化增强心脏收缩力的结果,而非相反。