Centre for Metabolic Bone Diseases, University of Sheffield, Sheffield, UK.
Mary McKillop Health Institute, Australian Catholic University, Melbourne, Australia.
Osteoporos Int. 2018 Aug;29(8):1747-1757. doi: 10.1007/s00198-018-4502-0. Epub 2018 Jun 12.
The present study, drawn from a sample of the Icelandic population, quantified high immediate risk and utility loss of subsequent fracture after a sentinel fracture (at the hip, spine, distal forearm and humerus) that attenuated with time.
The risk of a subsequent osteoporotic fracture is particularly acute immediately after an index fracture and wanes progressively with time. The aim of this study was to quantify the risk and utility consequences of subsequent fracture after a sentinel fracture (at the hip, spine, distal forearm and humerus) with an emphasis on the time course of recurrent fracture.
The Reykjavik Study fracture registration, drawn from a sample of the Icelandic population (n = 18,872), recorded all fractures of the participants from their entry into the study until December 31, 2012. Medical records for the participants were manually examined and verified. First sentinel fractures were identified. Subsequent fractures, deaths, 10-year probability of fracture and cumulative disutility using multipliers derived from the International Costs and Utilities Related to Osteoporotic fractures Study (ICUROS) were examined as a function of time after fracture, age and sex.
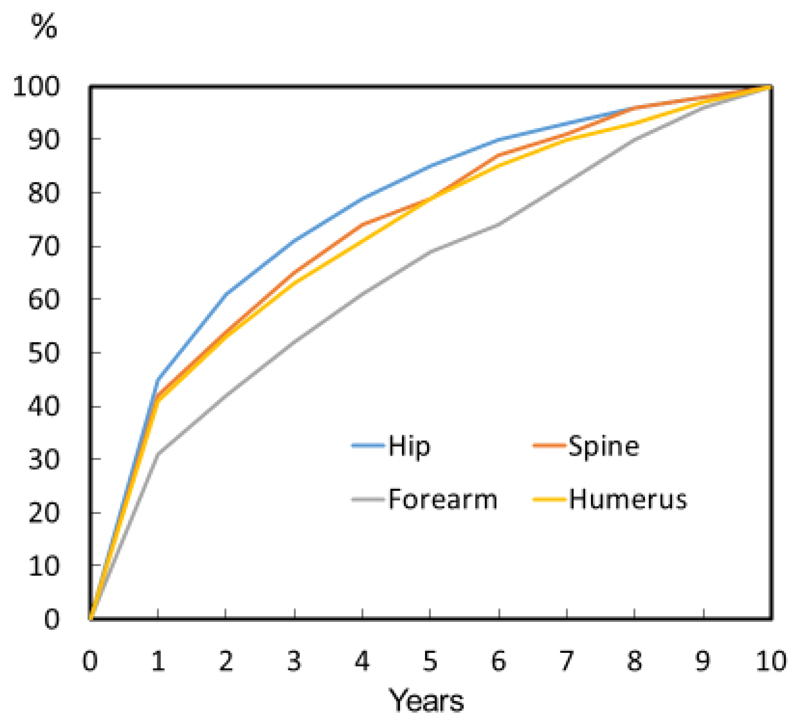
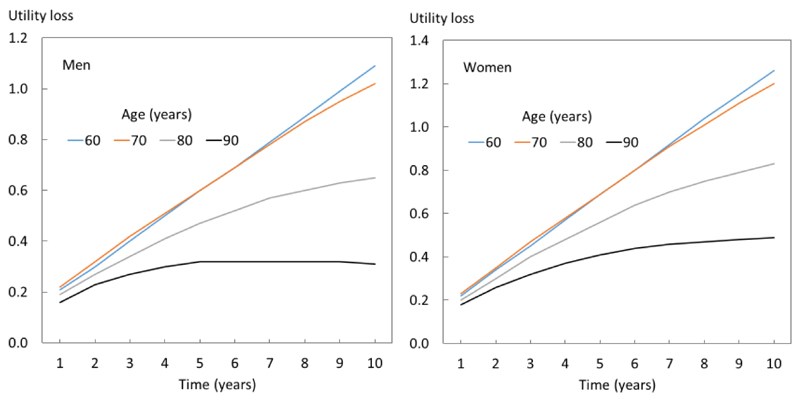
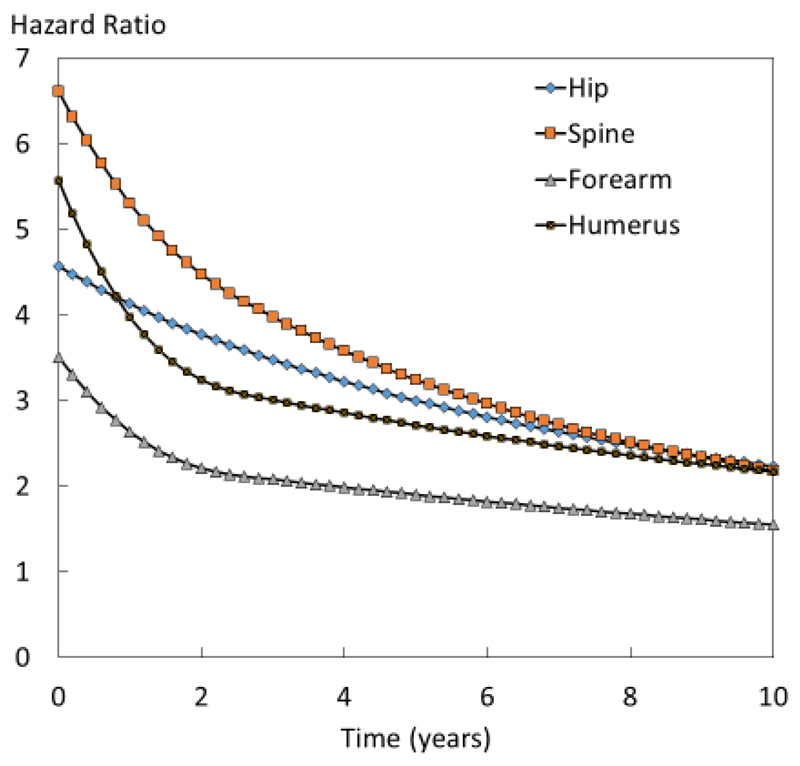
Over 10 years, subsequent fractures were sustained in 28% of 1498 individuals with a sentinel hip fracture. For other sentinel fractures, the proportion ranged from 35 to 38%. After each sentinel fracture, the risk of subsequent fracture was highest in the immediate post fracture interval and decreased markedly with time. Thus, amongst individuals who sustained a recurrent fracture, 31-45% did so within 1 year of the sentinel fracture. Hazard ratios for fracture recurrence (population relative risks) were accordingly highest immediately after the sentinel fracture (2.6-5.3, depending on the site of fracture) and fell progressively over 10 years (1.5-2.2). Population relative risks also decreased progressively with age. The utility loss during the first 10 years after a sentinel fracture varied by age (less with age) and sex (greater in women). In women at the age of 70 years, the mean utility loss due to fractures in the whole cohort was 0.081 whereas this was 12-fold greater in women with a sentinel hip fracture, and was increased 15-fold for spine fracture, 4-fold for forearm fracture and 8-fold for humeral fracture.
High fracture risks and utility loss immediately after fracture suggest that treatment given as soon as possible after fracture would avoid a higher number of new fractures compared with treatment given later. This provides the rationale for very early intervention immediately after a sentinel fracture.
本研究从冰岛人群中抽取样本,量化了哨兵骨折(髋部、脊柱、远端前臂和肱骨)后随后骨折的高即时风险和效用损失,并随时间衰减。
雷克雅未克研究骨折登记处从冰岛人群样本中抽取(n=18872),记录了参与者从进入研究到 2012 年 12 月 31 日的所有骨折情况。对参与者的病历进行了手动检查和验证。确定了首发哨兵骨折。随后的骨折、死亡、10 年骨折概率和使用国际骨质疏松症相关骨折成本和效用研究(ICUROS)得出的乘数累积的效用损失作为骨折后时间、年龄和性别的函数进行了检查。
在 10 年内,1498 名首发髋部骨折患者中有 28%发生了随后骨折。对于其他哨兵骨折,这一比例范围在 35%至 38%之间。在每次哨兵骨折后,随后骨折的风险在骨折后即刻间隔最高,并随时间显著下降。因此,在发生复发性骨折的患者中,31%-45%在首发骨折后 1 年内发生。骨折复发的风险比(人群相对风险)相应地在首发骨折后立即最高(2.6-5.3,取决于骨折部位),并在 10 年内逐渐下降(1.5-2.2)。人群相对风险也随年龄逐渐下降。首发骨折后 10 年内的效用损失因年龄(随年龄减小)和性别(女性更大)而异。在 70 岁的女性中,整个队列因骨折导致的平均效用损失为 0.081,而首发髋部骨折的女性这一数字是其 12 倍,脊柱骨折是其 15 倍,前臂骨折是其 4 倍,肱骨骨折是其 8 倍。
骨折后即刻高骨折风险和效用损失表明,与后期治疗相比,尽早给予骨折治疗将避免更多新骨折。这为哨兵骨折后立即进行早期干预提供了依据。
随后发生骨质疏松性骨折的风险在首发骨折后尤其急性,并随时间逐渐减弱。本研究的目的是量化首发骨折(髋部、脊柱、远端前臂和肱骨)后随后骨折的风险和效用后果,特别强调了复发性骨折的时间过程。
本研究从冰岛人群中抽取样本,量化了哨兵骨折(髋部、脊柱、远端前臂和肱骨)后随后骨折的高即时风险和效用损失,并随时间衰减。
首发骨折后,随后发生骨质疏松性骨折的风险尤其急性,并随时间逐渐减弱。本研究的目的是量化首发骨折(髋部、脊柱、远端前臂和肱骨)后随后骨折的风险和效用后果,特别强调了复发性骨折的时间过程。
雷克雅未克研究骨折登记处从冰岛人群样本中抽取(n=18872),记录了参与者从进入研究到 2012 年 12 月 31 日的所有骨折情况。对参与者的病历进行了手动检查和验证。确定了首发哨兵骨折。随后的骨折、死亡、10 年骨折概率和使用国际骨质疏松症相关骨折成本和效用研究(ICUROS)得出的乘数累积的效用损失作为骨折后时间、年龄和性别的函数进行了检查。
在 10 年内,1498 名首发髋部骨折患者中有 28%发生了随后骨折。对于其他哨兵骨折,这一比例范围在 35%至 38%之间。在每次哨兵骨折后,随后骨折的风险在骨折后即刻间隔最高,并随时间显著下降。因此,在发生复发性骨折的患者中,31%-45%在首发骨折后 1 年内发生。骨折复发的风险比(人群相对风险)相应地在首发骨折后立即最高(2.6-5.3,取决于骨折部位),并在 10 年内逐渐下降(1.5-2.2)。人群相对风险也随年龄逐渐下降。首发骨折后 10 年内的效用损失因年龄(随年龄减小)和性别(女性更大)而异。在 70 岁的女性中,整个队列因骨折导致的平均效用损失为 0.081,而首发髋部骨折的女性这一数字是其 12 倍,脊柱骨折是其 15 倍,前臂骨折是其 4 倍,肱骨骨折是其 8 倍。
骨折后即刻高骨折风险和效用损失表明,与后期治疗相比,尽早给予骨折治疗将避免更多新骨折。这为哨兵骨折后立即进行早期干预提供了依据。