Kimura Tomoki, Aikata Hiroshi, Doi Yoshiko, Imano Nobuki, Takeuchi Yuki, Takahashi Ippei, Nishibuchi Ikuno, Katsuta Tsuyoshi, Kenjo Masahiro, Murakami Yuji, Awai Kazuo, Chayama Kazuaki, Nagata Yasushi
1 Department of Radiation Oncology, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, Japan.
2 Division of Frontier Medical Science, Department of Medicine and Molecular Science, Programs for Biomedical Research, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, Japan.
Technol Cancer Res Treat. 2018 Jan 1;17:1533033818783450. doi: 10.1177/1533033818783450.
To compare the efficacy and safety of stereotactic body radiation therapy with or without transcatheter arterial chemoembolization for patients with small hepatocellular carcinoma who were ineligible for resection or ablation therapies.
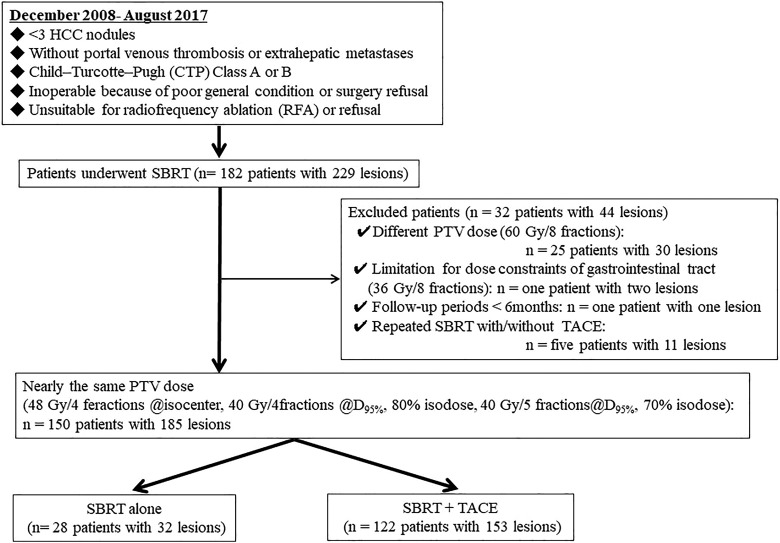
A total of 150 patients with 185 hepatocellular carcinoma (≤3 nodules, Child-Turcotte-Pugh class A or B, and no vascular or extrahepatic metastases) were treated with stereotactic body radiation therapy. In principle, transcatheter arterial chemoembolization was combined before stereotactic body radiation therapy (combination group), but some patients were treated with stereotactic body radiation therapy alone. The prescribed dose of stereotactic body radiation therapy was 48 Gy in 4 fractions at the isocenter and 40 Gy in 4 or 5 fractions at the dose covering 95% of the planning target volume. The overall survival, progression-free survival, local progression free survival, and complication rates were retrospectively compared between the groups. Local progression was defined as irradiated tumor growth in dynamic computed tomography follow-up. Tumor responses were assessed according to the Modified Response Evaluation Criteria in Solid Tumors. Treatment-related toxicities were evaluated according to the Common Terminology Criteria for Adverse Events version 4.0.
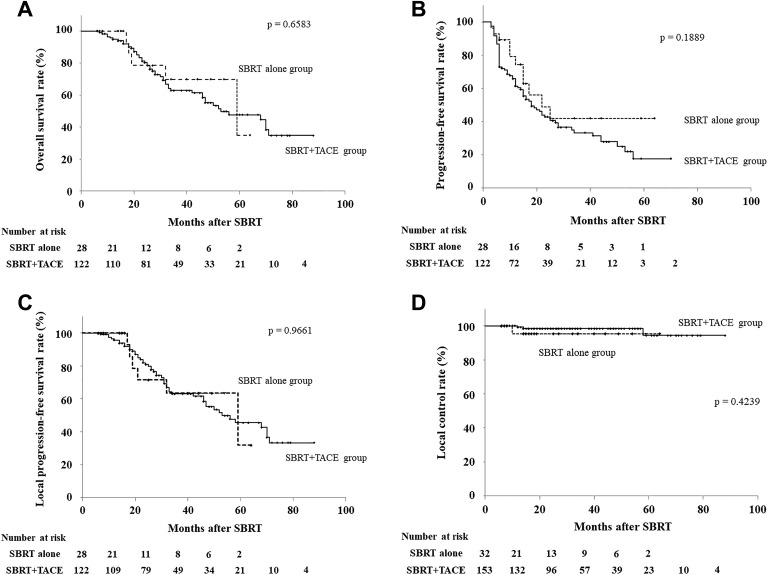
Twenty-eight and 122 patients were enrolled in the stereotactic body radiation therapy alone and combination groups, respectively. The median follow-up periods were 16 and 29 months, respectively. The 2-year overall, progression-free, and local progression-free survival times in stereotactic body radiation therapy alone and combination groups were 78.6% and 80.3% ( P = .6583), 49.0% and 42.9% ( P = .188), and 71.4% and 80.8% ( P = .9661), respectively. The incidence of ≥grade 3 toxicities was 17.9% in stereotactic body radiation therapy alone group and 18.9% in combination group ( P = .903).
Stereotactic body radiation therapy alone may be a good treatment option for patients with small hepatocellular carcinoma who were ineligible for resection or ablation therapies.
比较立体定向体部放射治疗联合或不联合经动脉化疗栓塞术治疗无法进行手术切除或消融治疗的小肝癌患者的疗效和安全性。
共有150例患有185个肝细胞癌(≤3个结节,Child-Turcotte-Pugh A或B级,无血管或肝外转移)的患者接受了立体定向体部放射治疗。原则上,在立体定向体部放射治疗前联合经动脉化疗栓塞术(联合组),但部分患者仅接受了立体定向体部放射治疗。立体定向体部放射治疗的处方剂量为等中心处48 Gy分4次给予,剂量覆盖95%计划靶体积处40 Gy分4或5次给予。回顾性比较两组的总生存期、无进展生存期、局部无进展生存期和并发症发生率。局部进展定义为动态计算机断层扫描随访中照射部位肿瘤生长。根据实体瘤改良反应评估标准评估肿瘤反应。根据不良事件通用术语标准第4.0版评估治疗相关毒性。
单纯立体定向体部放射治疗组和联合组分别纳入28例和122例患者。中位随访期分别为16个月和29个月。单纯立体定向体部放射治疗组和联合组的2年总生存期、无进展生存期和局部无进展生存期分别为78.6%和80.3%(P = 0.6583)、49.0%和42.9%(P = 0.188)、71.4%和80.8%(P = 0.9661)。单纯立体定向体部放射治疗组≥3级毒性发生率为17.9%,联合组为18.9%(P = 0.903)。
对于无法进行手术切除或消融治疗的小肝癌患者,单纯立体定向体部放射治疗可能是一种较好的治疗选择。