Unidad Médico-Quirúrgica de Enfermedades Respiratorias, Instituto de Biomedicina de Sevilla (IBiS), Hospital Universitario Virgen del Rocío/Universidad de Sevilla, Avda. Manuel Siurot, s/n, 41013, Seville, Spain.
UGC-DCCU Bahía de Cádiz-La Janda, Cadiz, Spain.
BMC Med Res Methodol. 2018 Jul 3;18(1):68. doi: 10.1186/s12874-018-0528-4.
A thorough evaluation of the adequacy of clinical practice in a designated health care setting and temporal context is key for clinical care improvement. This study aimed to perform a clinical audit of primary care to evaluate clinical care delivered to patients with COPD in routine clinical practice.
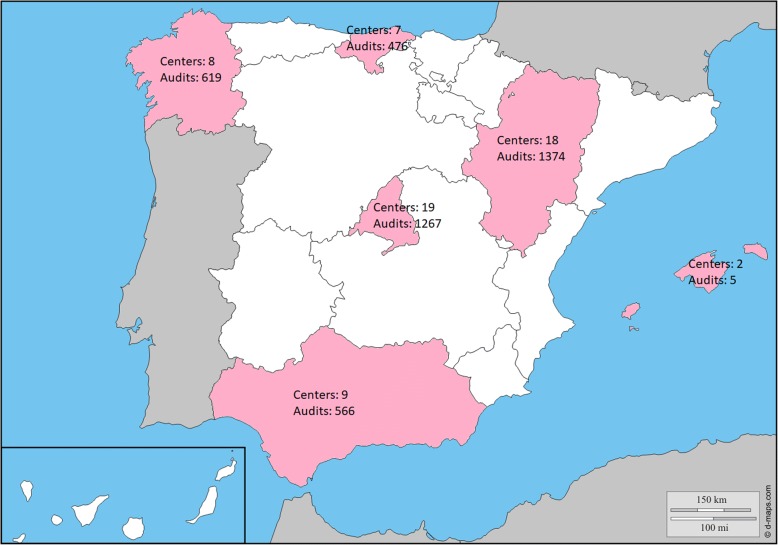
The Community Assessment of COPD Health Care (COACH) study was an observational, multicenter, nationwide, non-interventional, retrospective, clinical audit of randomly selected primary care centers in Spain. Two different databases were built: the resources and organization database and the clinical database. From January 1, 2015 to December 31, 2016 consecutive clinical cases of COPD in each participating primary care center (PCC) were audited. For descriptive purposes, we collected data regarding the age at diagnosis of COPD and the age at audit, gender, the setting of the PCC (rural/urban), and comorbidities for each patient. Two guidelines widely and uniformly used in Spain were carefully reviewed to establish a benchmark of adequacy for the audited cases. Clinical performance was analyzed at the patient, center, and regional levels. The degree of adequacy was categorized as excellent (> 80%), good (60-80%), adequate (40-59%), inadequate (20-39%), and highly inadequate (< 20%).
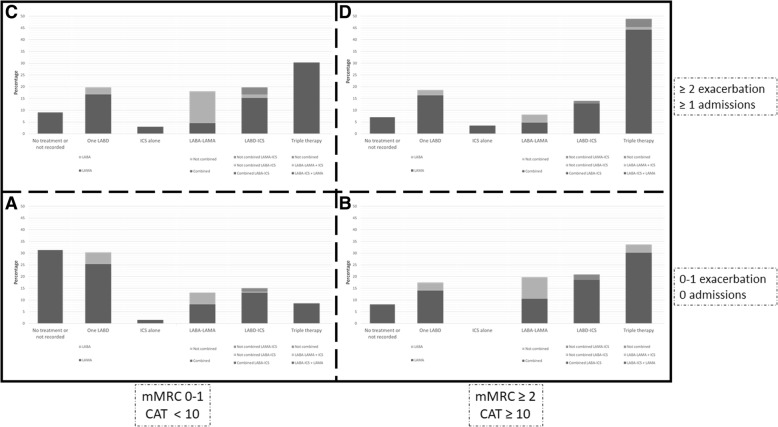
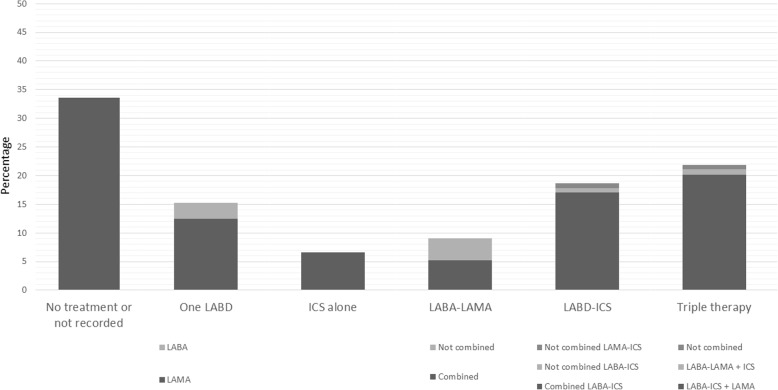
During the study 4307 cases from 63 primary care centers in 6 regions of the country were audited. Most evaluated parameters were judged to fall in the inadequate performance category. A correct diagnosis based on previous exposure plus spirometric obstruction was made in an average of 17.6% of cases, ranging from 9.8 to 23.3% depending on the region. During the audited visit, only 67 (1.6%) patients had current post-bronchodilator obstructive spirometry; 184 (4.3%) patients had current post-bronchodilator obstructive spirometry during either the audited or initial diagnostic visit. Evaluation of dyspnea was performed in 11.1% of cases. Regarding treatment, 33.6% received no maintenance inhaled therapies (ranging from 31.3% in GOLD A to 7.0% in GOLD D). The two most frequently registered items were exacerbations in the previous year (81.4%) and influenza vaccination (87.7%).
The results of this audit revealed a large variability in clinical performance across centers, which was not fully attributable to the severity of the disease.
彻底评估指定医疗保健环境和时间背景下的临床实践是否充分,是改善临床护理的关键。本研究旨在对初级保健进行临床审核,以评估常规临床实践中为 COPD 患者提供的临床护理。
社区 COPD 保健评估(COACH)研究是一项观察性、多中心、全国性、非干预性、回顾性、随机选择西班牙初级保健中心的临床审核。建立了两个不同的数据库:资源和组织数据库和临床数据库。从 2015 年 1 月 1 日至 2016 年 12 月 31 日,对每个参与的初级保健中心(PCC)的连续 COPD 临床病例进行审核。为了描述目的,我们收集了每个患者的 COPD 诊断年龄和审核年龄、性别、PCC 的设置(农村/城市)以及合并症的数据。仔细审查了在西班牙广泛和统一使用的两份指南,以确定审核病例的充分性基准。在患者、中心和地区层面分析了临床绩效。充分性程度分为优秀(>80%)、良好(60-80%)、充分(40-59%)、不充分(20-39%)和高度不充分(<20%)。
在研究期间,从该国 6 个地区的 63 个初级保健中心审核了 4307 例病例。评估的大多数参数被认为属于表现不佳类别。根据以前的暴露加肺功能阻塞,平均有 17.6%的病例做出了正确诊断,根据地区的不同,范围在 9.8%至 23.3%之间。在审核访问期间,只有 67 名(1.6%)患者有当前支气管扩张后阻塞性肺功能;184 名(4.3%)患者在审核或初始诊断访问期间有当前支气管扩张后阻塞性肺功能。对呼吸困难的评估在 11.1%的病例中进行。关于治疗,33.6%的患者未接受维持性吸入治疗(范围从 GOLD A 的 31.3%到 GOLD D 的 7.0%)。记录最频繁的两个项目是前一年的加重(81.4%)和流感疫苗接种(87.7%)。
该审核的结果显示,各中心之间的临床绩效存在很大差异,这并不能完全归因于疾病的严重程度。