Chen Xueping, Wei Qian-Qian, Chen Yongping, Cao Bei, Ou RuWei, Hou Yanbing, Yuan Xiaoqin, Zhang Lingyu, Liu Hui, Shang Huifang
Department of Neurology, West China Hospital, Sichuan University, Chengdu, China.
Front Neurol. 2018 Jun 19;9:442. doi: 10.3389/fneur.2018.00442. eCollection 2018.
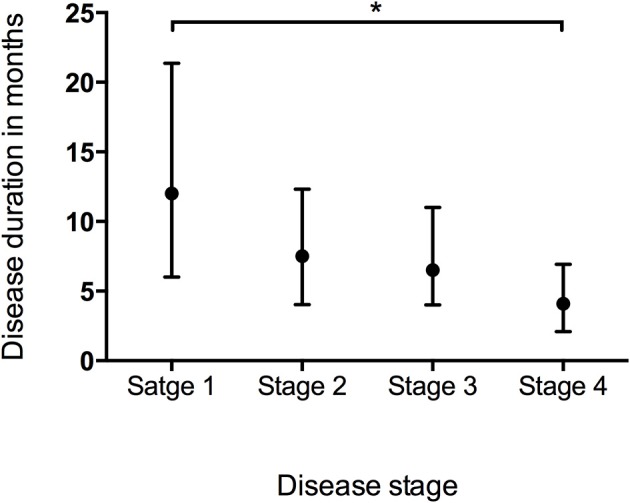
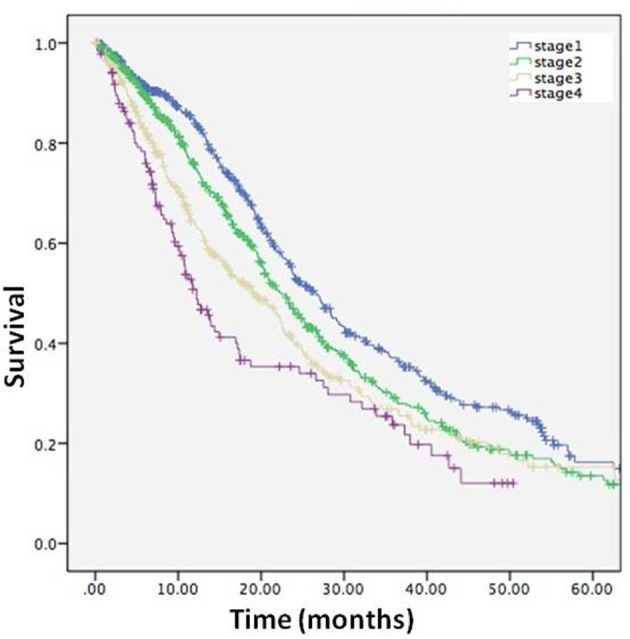
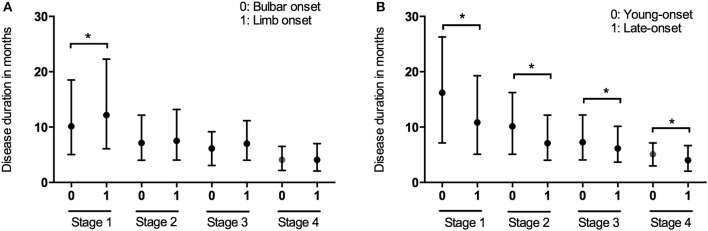
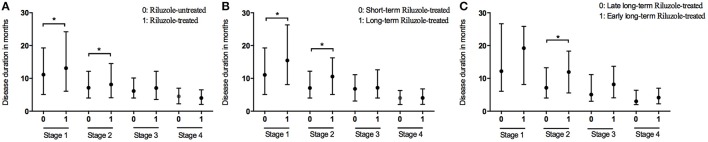
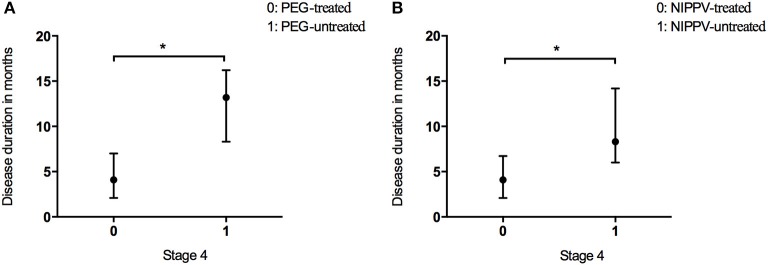
It is important to explore the utility of clinical staging systems in the management of amyotrophic lateral sclerosis (ALS). Our aim was to assess the validity of King's College in a Chinese ALS cohort, by evaluating the duration and informativeness of each stage and examining the association between stage and prognosis. From May 2008 to December 2016, patients with a likely diagnosis of ALS were registered. We prospectively assessed the progression of the patients through the stages and calculated the duration of each stage. The median duration in Stage 1 was 12.00 months, Stage 2 7.50 months, Stage 3 6.50 months, and Stage 4 4.10 months. Subset analysis revealed that the spinal-onset and early-onset patients had a longer median time in Stage 1 compared to bulbar-onset and late-onset patients, respectively. Riluzole treatment extended the durations of Stages 1 and 2, and the effect was maintained in patients with long-term use of riluzole (>6 months). Patients who initiated long-term riluzole therapy early, in Stage 1 or 2, had a longer Stage 2. Patients who received percutaneous gastrostomy endoscopy (PEG) or non-invasive positive-pressure ventilation (NIPPV) showed longer durations of Stage 4. The differences in survival time measured from each stage to death or censor date were significant. We validated the King's College staging system in a Chinese population, and showed this system to be useful in clinical practice. Patients with bulbar-onset or an age of onset>45 years tended to have rapidly progressing ALS. Riluzole may be more effective when initiated in an early disease stage and continued long-term. PEG and NIPPV treatments can extend disease duration of Stage 4.
探索临床分期系统在肌萎缩侧索硬化症(ALS)管理中的效用非常重要。我们的目的是通过评估每个阶段的持续时间和信息量,并研究阶段与预后之间的关联,来评估国王学院分期系统在中国ALS队列中的有效性。2008年5月至2016年12月,对疑似ALS的患者进行了登记。我们前瞻性地评估了患者在各阶段的进展情况,并计算了每个阶段的持续时间。1期的中位持续时间为12.00个月,2期为7.50个月,3期为6.50个月,4期为4.10个月。亚组分析显示,与延髓起病和晚发性患者相比,脊髓起病和早发性患者在1期的中位时间更长。利鲁唑治疗延长了1期和2期的持续时间,且长期使用利鲁唑(>6个月)的患者维持了这种效果。在1期或2期早期开始长期利鲁唑治疗的患者,2期更长。接受经皮胃造瘘内镜检查(PEG)或无创正压通气(NIPPV)的患者4期持续时间更长。从每个阶段到死亡或审查日期测量的生存时间差异显著。我们在中国人群中验证了国王学院分期系统,并表明该系统在临床实践中有用。延髓起病或发病年龄>45岁的患者往往患有进展迅速的ALS。利鲁唑在疾病早期开始并长期持续使用时可能更有效。PEG和NIPPV治疗可延长4期的疾病持续时间。