Policy Research Unit in Maternal Health and Care, National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, Oxford, UK.
School of Health Sciences, City, University of London, London, UK.
J Epidemiol Community Health. 2018 Oct;72(10):911-918. doi: 10.1136/jech-2018-210453. Epub 2018 Jul 4.
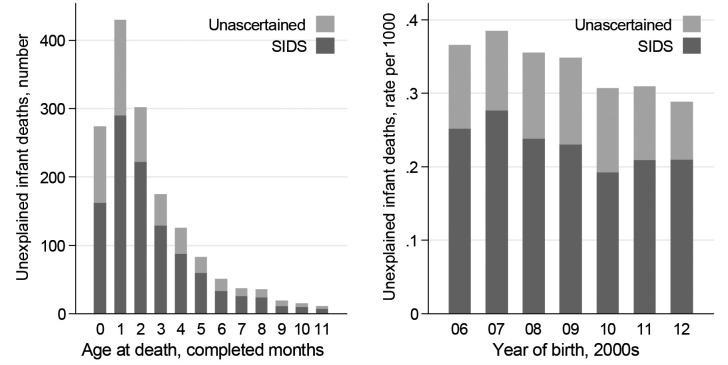
Unexplained deaths in infancy comprise 'sudden infant death syndrome' (SIDS) and deaths without ascertained cause. They are typically sleep-related, perhaps triggered by unsafe sleep environments. Preterm birth may increase risk, and varies with ethnicity. We aimed to compare ethnic-specific rates of unexplained infant death, explore sociodemographic explanations for ethnic variation, and examine the role of preterm birth.
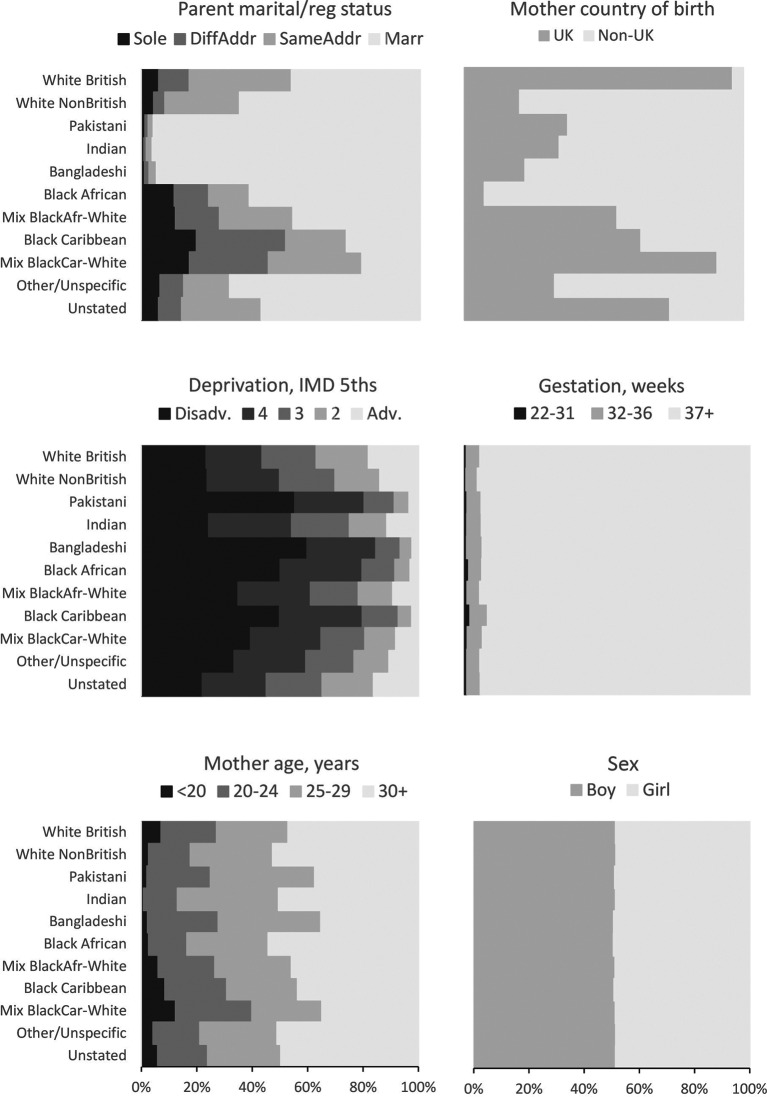
We analysed routine data for 4.6 million live singleton births in England and Wales 2006-2012, including seven non-White ethnic groups ranging in size from 29 313 (Mixed Black-African-White) to 180 265 (Pakistani). We calculated rates, birth-year-adjusted ORs, and effects of further adjustments on the χ for ethnic variation.
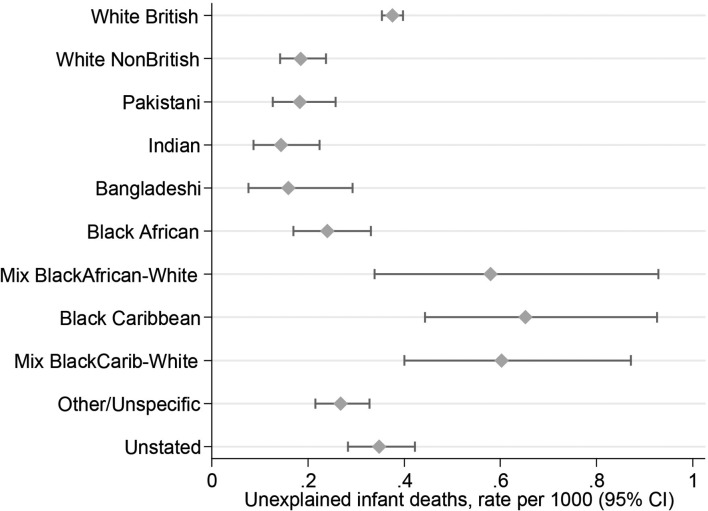
There were 1559 unexplained infant deaths. Crude rates per 1000 live singleton births were as follows: 0.1-0.2 for Indian, Bangladeshi, Pakistani, White Non-British, Black African; 0.4 for White British; 0.6-0.7 for Mixed Black-African-White, Mixed Black-Caribbean-White, Black Caribbean. Birth-year-adjusted ORs relative to White British ranged from 0.38 (95% CI 0.24 to 0.60) for Indian babies to 1.73 (1.21 to 2.47) for Black Caribbean (χ(10 df)=113.6, p<0.0005). Combined adjustment for parents' marital/registration status and mother's country of birth (UK/non-UK) attenuated the ethnic variation. Adjustments for gestational age at birth, maternal age and area deprivation made little difference.
Substantial ethnic disparity in risk of unexplained infant death exists in England and Wales. Apparently not attributable to preterm birth or area deprivation, this may reflect cultural differences in infant care. Further research into infant-care practices in low-risk ethnic groups might enable more effective prevention of such deaths in the general population.
婴儿不明原因死亡包括“婴儿猝死综合征”(SIDS)和死因不明的死亡。它们通常与睡眠有关,可能是由不安全的睡眠环境引发的。早产可能会增加风险,且风险因种族而异。我们旨在比较婴儿不明原因死亡的特定种族率,探讨社会人口因素对种族差异的解释,并研究早产的作用。
我们分析了 2006 年至 2012 年英格兰和威尔士 460 万例活产单胎的数据,包括七个不同种族群体,规模从 29313 人(混合黑-非裔-白种人)到 180265 人(巴基斯坦人)不等。我们计算了比率、出生年份调整后的比值比(OR)以及进一步调整对种族差异 χ 的影响。
有 1559 例婴儿不明原因死亡。每 1000 例活产单胎的粗死亡率如下:印度人、孟加拉国人、巴基斯坦人、白人非英国人、黑人非洲人为 0.1-0.2;白人为 0.4;混血黑-非裔-白种人、混血黑-加勒比-白种人、黑人加勒比人为 0.6-0.7。与白种英国人相比,印度婴儿的出生年份调整后的 OR 范围为 0.38(95%CI 0.24 至 0.60),而黑人加勒比人的 OR 为 1.73(1.21 至 2.47)(χ(10df)=113.6,p<0.0005)。联合调整父母的婚姻/注册状况和母亲的出生国(英国/非英国)减弱了种族差异。调整出生时的胎龄、母亲年龄和地区贫困程度对差异影响不大。
在英格兰和威尔士,婴儿不明原因死亡的风险存在显著的种族差异。这种差异显然不是由于早产或地区贫困造成的,可能反映了婴儿护理方面的文化差异。对低风险种族群体的婴儿护理实践进行进一步研究,可能有助于更有效地预防一般人群中此类死亡事件的发生。