Unicomb Leanne, Begum Farzana, Leontsini Elli, Rahman Mahbubur, Ashraf Sania, Naser Abu Mohd, Nizame Fosiul A, Jannat Kaniz, Hussain Faruqe, Parvez Sarker Masud, Arman Shaila, Mobashara Moshammot, Luby Stephen P, Winch Peter J
Infectious Disease Division, Environmental Intervention Unit, Enteric and Respiratory Disease Program, International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), 68 Shahed Tajuddin Ahmed Sarani, Mohakhali, Dhaka, 1212, Bangladesh.
Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Trials. 2018 Jul 6;19(1):359. doi: 10.1186/s13063-018-2709-1.
Water, sanitation, and hygiene (WASH) efficacy trials deliver interventions to the target population under optimal conditions to estimate their effects on outcomes of interest, to inform subsequent selection for inclusion in routine programs. A systematic and intensive approach to intervention delivery is required to achieve the high-level uptake necessary to measure efficacy. We describe the intervention delivery system adopted in the WASH Benefits Bangladesh study, as part of a three-paper series on WASH Benefits Intervention Delivery and Performance.
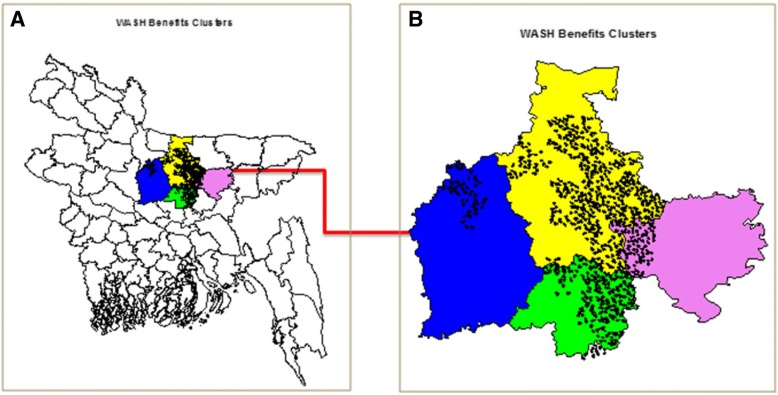
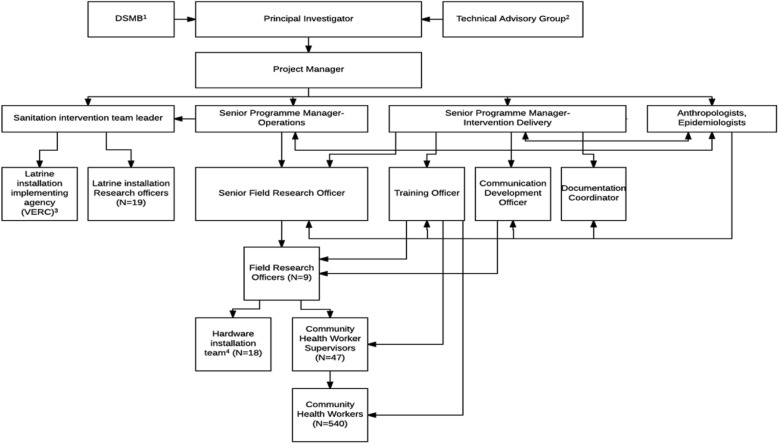
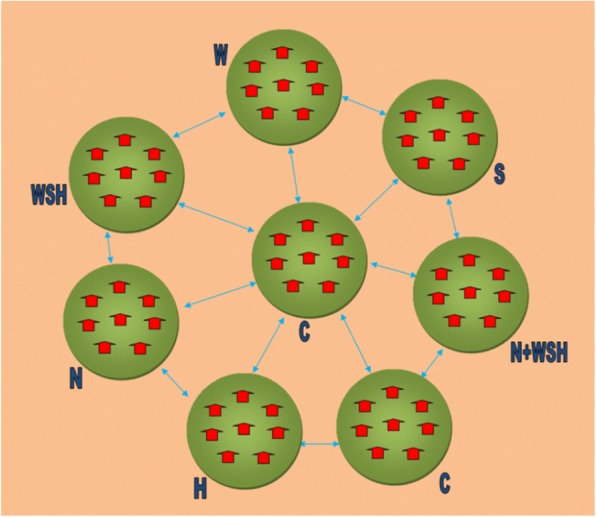
Community Health Workers (CHWs) delivered individual and combined WASH and nutrition interventions to 4169 enrolled households in geographically matched clusters. Households were provided with free enabling technologies and supplies, integrated with parallel behaviour-change promotion. Behavioural objectives were drinking treated, safely stored water, safe feces disposal, handwashing with soap at key times, and age-appropriate nutrition behaviours (birth to 24 months). The intervention delivery system built on lessons learned from prior WASH intervention effectiveness, implementation, and formative research studies. We recruited local CHWs, residents of the study villages, through transparent merit-based selection methods, and consultation with community leaders. CHW supervisors received training on direct intervention delivery, then trained their assigned CHWs. CHWs in turn used the technologies in their own homes. Each CHW counseled six to eight intervention households spread across a 0.2-2.2-km radius, with a 1:12 supervisor-to-CHW ratio. CHWs met monthly with supervisor-trainers to exchange experiences and adapt technology and behaviour-change approaches to evolving conditions. Intervention uptake was tracked through fidelity measures, with a priori benchmarks necessary for an efficacy study.
Sufficient levels of uptake were attained by the fourth intervention assessment month and sustained throughout the intervention period. Periodic internal CHW monitoring resulted in discontinuation of a small number of low performers.
The intensive intervention delivery system required for an efficacy trial differs in many respects from the system for a routine program. To implement a routine program at scale requires further research on how to optimize the supervisor-to-CHW-to-intervention household ratios, as well as other program costs without compromising program effectiveness.
ClinicalTrials.gov, ID: NCC01590095 . Registered on 2 May 2012.
水、环境卫生和个人卫生(WASH)功效试验在最佳条件下向目标人群提供干预措施,以评估其对感兴趣的结果的影响,为随后纳入常规项目的选择提供依据。需要一种系统且密集的干预措施实施方法,以实现测量功效所需的高接受率。我们描述了“孟加拉国WASH效益研究”中采用的干预措施实施系统,这是关于WASH效益干预措施实施与效果的三篇系列论文的一部分。
社区卫生工作者(CHW)向地理匹配群组中的4169户登记家庭提供单独及综合的WASH和营养干预措施。为家庭提供免费的支持技术和用品,并结合并行的行为改变促进措施。行为目标包括饮用经过处理、安全储存的水,安全处理粪便,在关键时间用肥皂洗手,以及适合年龄的营养行为(出生至24个月)。干预措施实施系统借鉴了先前WASH干预效果、实施及形成性研究的经验教训。我们通过基于功绩的透明选拔方法,并与社区领袖协商,招募了当地的CHW(研究村庄的居民)。CHW监督员接受了直接干预措施实施方面的培训,然后培训他们所负责的CHW。CHW继而在自己家中使用这些技术。每名CHW为半径0.2至2.2公里范围内的6至8户干预家庭提供咨询,监督员与CHW的比例为1:12。CHW每月与担任培训师的监督员会面,交流经验,并根据不断变化的情况调整技术和行为改变方法。通过保真度测量跟踪干预措施的接受情况,这是功效研究所需的先验基准。
在第四个干预评估月达到了足够的接受水平,并在整个干预期内保持。定期的内部CHW监测导致少数表现不佳者被终止。
功效试验所需的密集干预措施实施系统在许多方面与常规项目系统不同。要大规模实施常规项目,需要进一步研究如何在不影响项目效果的情况下优化监督员与CHW与干预家庭的比例,以及其他项目成本。
ClinicalTrials.gov,ID:NCC01590095。于2012年5月2日注册。