Divisions of Renal Diseases and Hypertension and.
Biostatistics, University of Minnesota, Minneapolis, Minnesota.
Clin J Am Soc Nephrol. 2018 Sep 7;13(9):1348-1357. doi: 10.2215/CJN.13181117. Epub 2018 Jul 5.
Ambulatory BP is increasingly recognized as a better measure of the risk for adverse outcomes related to hypertension, an important comorbidity in patients with CKD. Varying definitions of white-coat and masked hypertension have made it difficult to evaluate differences in prevalence of these BP patterns across CKD cohorts.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: The International Database of Ambulatory BP in Renal Patients collaborative group established a large database of demographic, clinical, and ambulatory BP data from patients with CKD from cohorts in Italy, Spain, the Chronic Renal Insufficiency Cohort (CRIC) and the African American Study of Kidney Disease and Hypertension Cohort Study (AASK) in the United States, and the CKD Japan Cohort (CKD-JAC). Participants (=7518) with CKD were included in the present analyses. Cutoffs for defining controlled BP were 140/90 mm Hg for clinic and 130/80 mm Hg for 24-hour ambulatory BP.
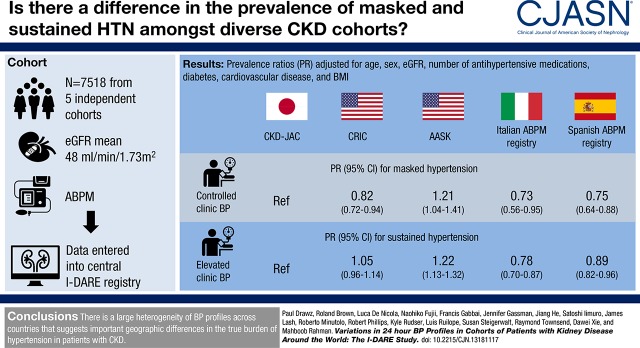
Among those with controlled clinic BP, compared with CKD-JAC, AASK participants were more likely to have masked hypertension (prevalence ratio [PR], 1.21; 95% confidence interval [95% CI], 1.04 to 1.41) whereas CRIC (PR, 0.82; 0.72 to 0.94), Italian (PR, 0.73; 0.56 to 0.95), and Spanish participants (PR, 0.75; 0.64 to 0.88) were less likely. Among those with elevated clinic BP, AASK participants were more likely to have sustained hypertension (PR, 1.22; 95% CI, 1.13 to 1.32) whereas Italian (PR, 0.78; 0.70 to 0.87) and Spanish participants (PR, 0.89; 0.82 to 0.96) were less likely, although CRIC participants had similar prevalence as CKD-JAC. Prevalence of masked and sustained hypertension was elevated in males, patients with diabetes, participants on four or more antihypertensives, and those with moderate-to-severe proteinuria.
In a large, multinational database, the prevalence of masked and sustained hypertension varied across cohorts independent of important comorbidities.
动态血压监测越来越被认为是评估高血压相关不良结局风险的更好方法,高血压是慢性肾脏病患者的一个重要合并症。白大衣高血压和隐蔽性高血压的不同定义使得评估这些血压模式在不同慢性肾脏病患者队列中的发生率变得困难。
设计、地点、参与者和测量方法:国际肾脏动态血压数据库协作组建立了一个来自意大利、西班牙、慢性肾脏病队列研究(CRIC)和美国非洲裔美国人肾脏病和高血压队列研究(AASK)以及日本慢性肾脏病队列研究(CKD-JAC)的慢性肾脏病患者的大型人口统计学、临床和动态血压数据库。本研究纳入了患有慢性肾脏病的 7518 名参与者。诊室血压控制的定义为 140/90mmHg,24 小时动态血压控制的定义为 130/80mmHg。
在诊室血压得到控制的人群中,与 CKD-JAC 相比,AASK 参与者更有可能患有隐蔽性高血压(患病率比 [PR],1.21;95%置信区间 [95%CI],1.04 至 1.41),而 CRIC(PR,0.82;0.72 至 0.94)、意大利(PR,0.73;0.56 至 0.95)和西班牙参与者(PR,0.75;0.64 至 0.88)则不太可能。在诊室血压升高的人群中,AASK 参与者更有可能患有持续性高血压(PR,1.22;95%CI,1.13 至 1.32),而意大利(PR,0.78;0.70 至 0.87)和西班牙参与者(PR,0.89;0.82 至 0.96)则不太可能,尽管 CRIC 参与者的患病率与 CKD-JAC 相似。男性、患有糖尿病的患者、服用四种或更多种降压药的患者以及有中重度蛋白尿的患者中,隐蔽性高血压和持续性高血压的患病率较高。
在一个大型的、多国的数据库中,隐蔽性高血压和持续性高血压的患病率在不同队列中有所不同,这与重要的合并症无关。