Department of Neurosurgery, the First Affiliated Hospital of Nanchang University, No.17 Yongwai Street, Nanchang, Jiangxi Province, 330006, People's Republic of China.
Department of Pathology, the First Affiliated Hospital of Nanchang University, Nanchang, People's Republic of China.
Sci Rep. 2018 Jul 5;8(1):10215. doi: 10.1038/s41598-018-28282-4.
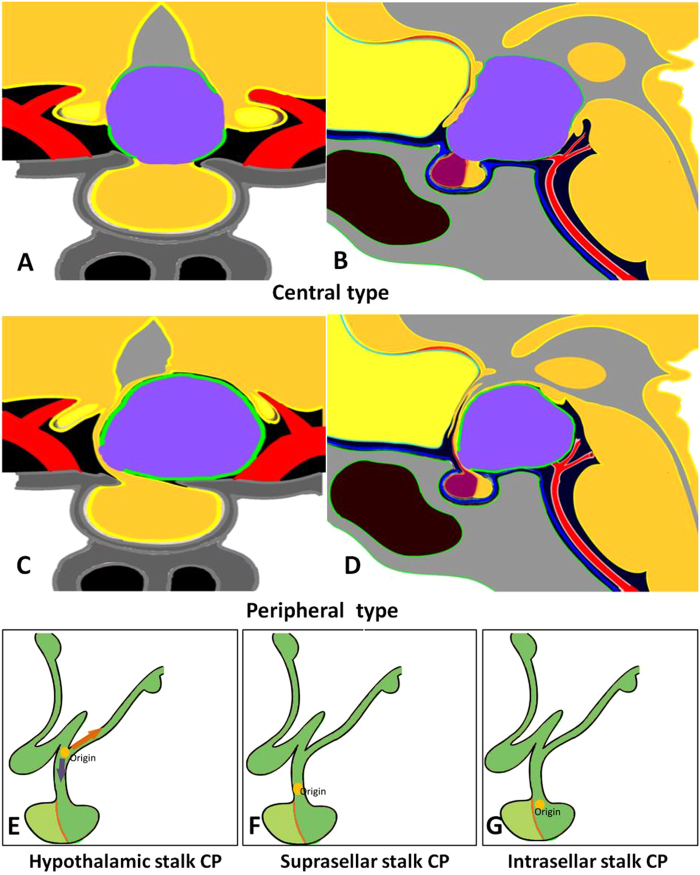
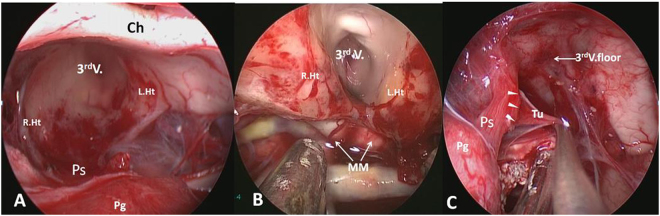
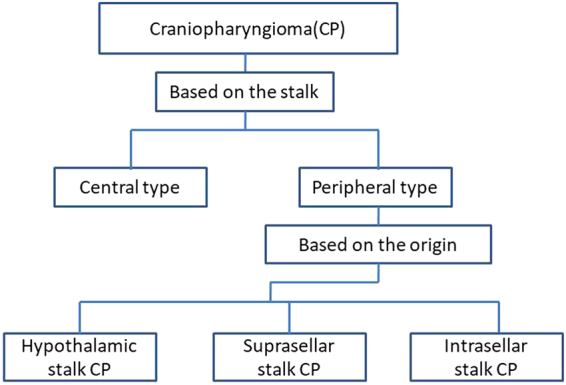
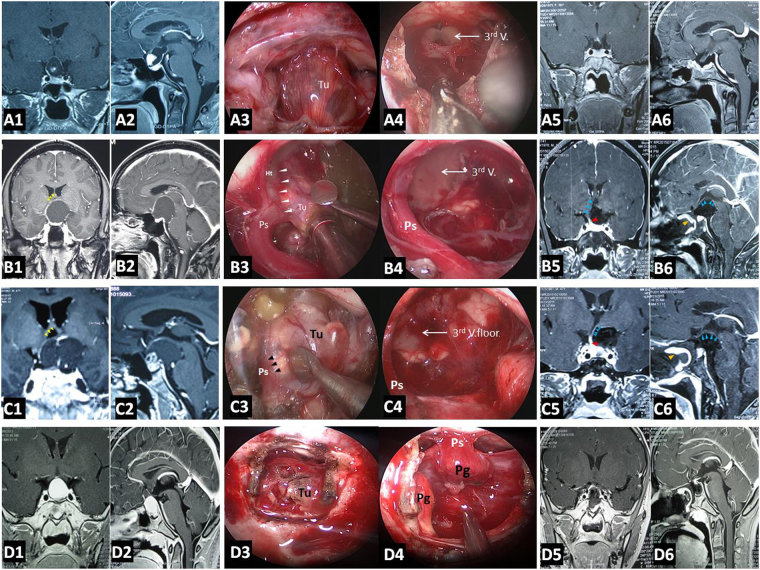
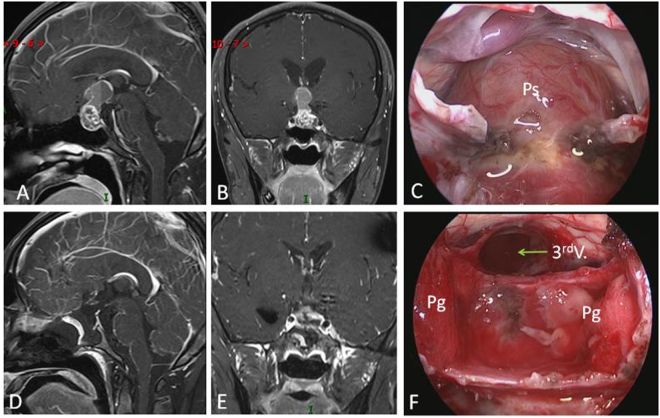
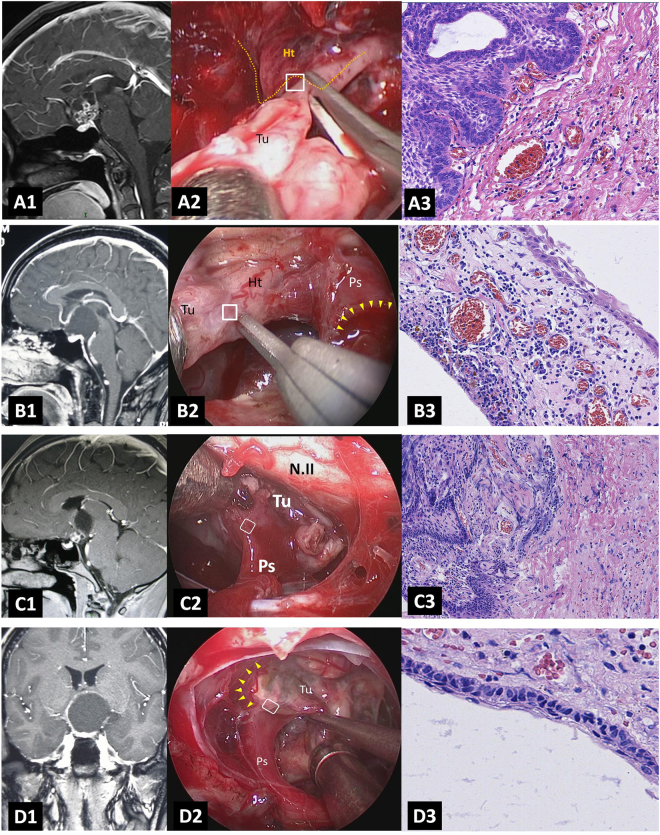
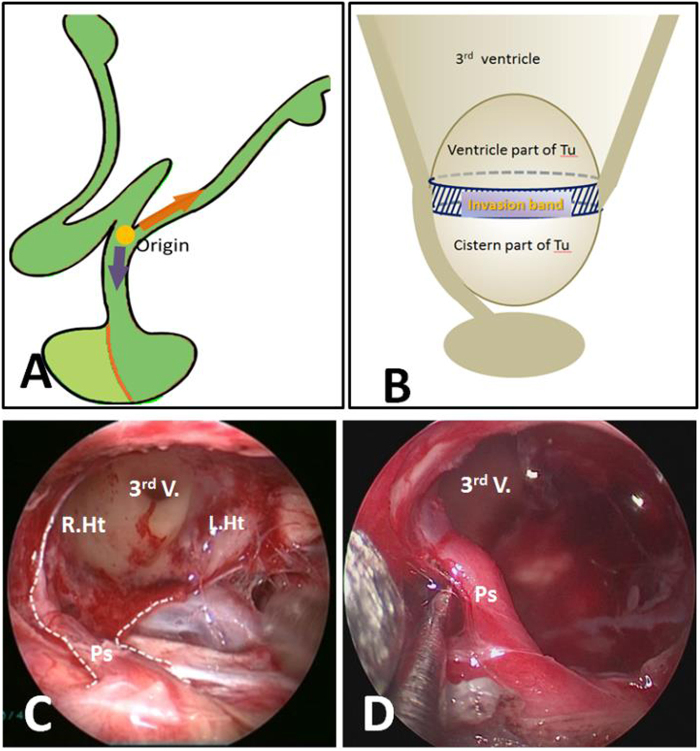
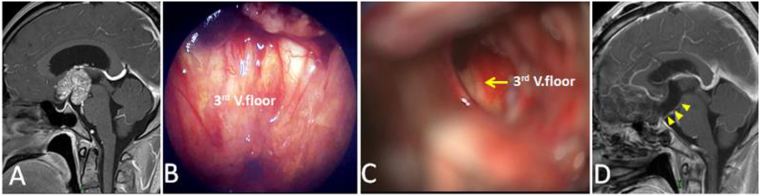
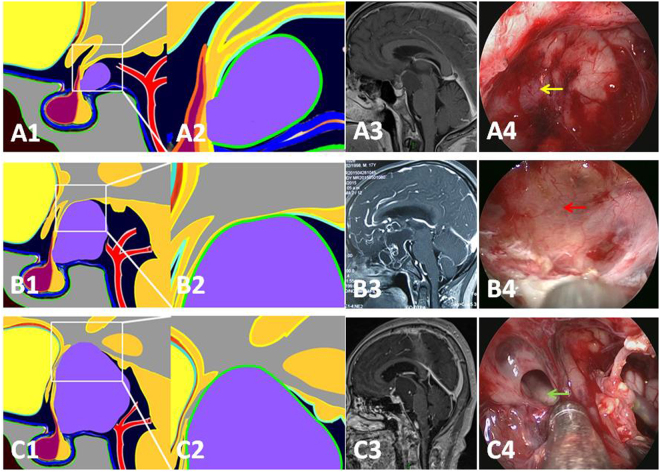
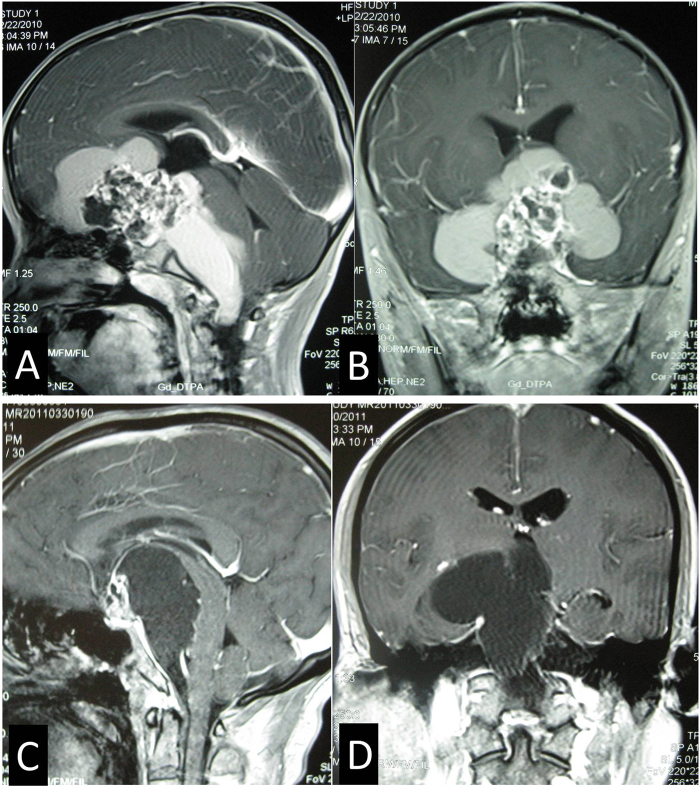
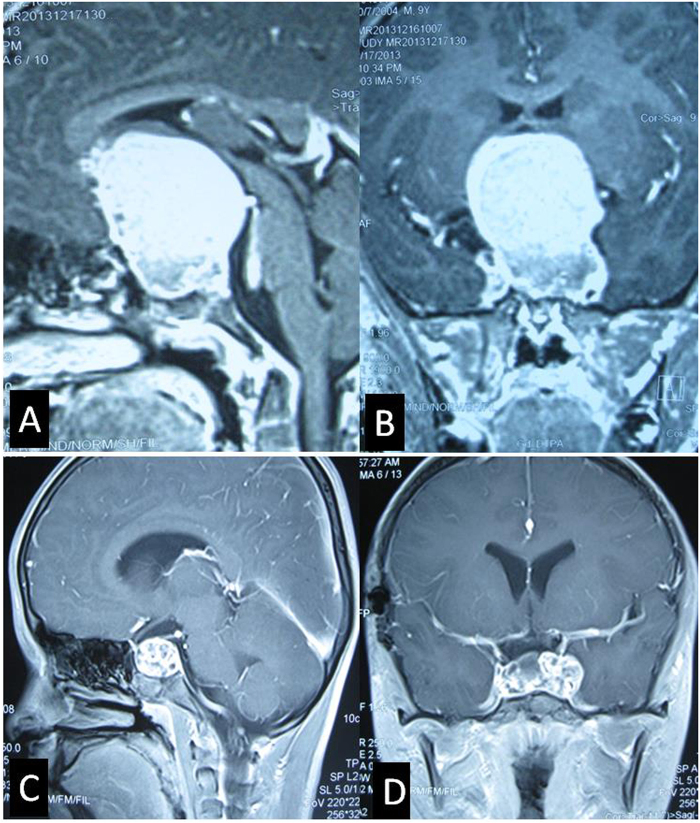
Endoscopic endonasal approach for craniopharyngioma (CP) resection provides a wide view and direct observation of hypothalamus and origin of tumor. Under endoscopy, 92 CPs were classified into 2 types: Peripheral and Central, according to its relation to pituitary stalk. Peripheral type was further divided into 3 subtypes: Hypothalamic stalk, Suprasellar stalk and Intrasellar stalk CP, according to the different origin site along hypothalamus-pituitary axis. Peripheral type arisen from the stalk but expanded and grown laterally in an exophytic pattern, accounting for 71.7% of all CPs, preservation rate of stalk was higher (76.0%). Central type grew within and along pituitary stalk and located strictly in the midline. The pituitary stalk was hardly preserved (only15.4%). Hypothalamic stalk CPs (n = 36, 54.6%) developed from the junction of hypothalamus and stalk, hypothalamus damage was found in all of this subtype after surgery. Suprasellar stalk CPs (n = 14, 21.2%) originated from the lower portion of stalk and displaced hypothalamus upward rather than infiltrated it. Intrasellar stalk CPs (n = 16, 24.2%) arose from the subdiaphragma portion of the stalk, with less hypothalamus damage. Recoginzing the origin of CP is helpful to understand its growth pattern and relation to hypothalamus, which is critical in planning the most appropriate surgical approach and degree of excision.
经鼻内镜颅咽管瘤切除术(endoscopic endonasal approach for craniopharyngioma resection, EEACR)提供了广泛的视野和对下丘脑及肿瘤起源的直接观察。在内镜下,92 例颅咽管瘤根据其与垂体柄的关系分为 2 型:外周型和中央型。外周型进一步根据其起源于下丘脑-垂体轴的不同部位分为 3 个亚型:下丘脑柄型、鞍上柄型和鞍内柄型颅咽管瘤。外周型起源于垂体柄,但以向外生长的方式扩张,占所有颅咽管瘤的 71.7%,保留垂体柄的比例较高(76.0%)。中央型在垂体柄内和沿其生长,严格位于中线。垂体柄几乎无法保留(仅 15.4%)。下丘脑柄型颅咽管瘤(n=36,54.6%)起源于下丘脑和垂体柄的交界处,该亚型术后均发现下丘脑损伤。鞍上柄型颅咽管瘤(n=14,21.2%)起源于垂体柄的下部,将下丘脑向上移位而不是浸润。鞍内柄型颅咽管瘤(n=16,24.2%)起源于垂体柄的亚膈部分,下丘脑损伤较少。识别颅咽管瘤的起源有助于了解其生长模式及其与下丘脑的关系,这对制定最合适的手术入路和切除程度至关重要。