Matsuo Takayuki, Kamada Kensaku, Izumo Tsuyoshi, Nagata Izumi
Department of Neurosurgery, Nagasaki University School of Medicine.
Neurol Med Chir (Tokyo). 2014;54(12):974-82. doi: 10.2176/nmc.oa.2014-0038. Epub 2014 Nov 29.
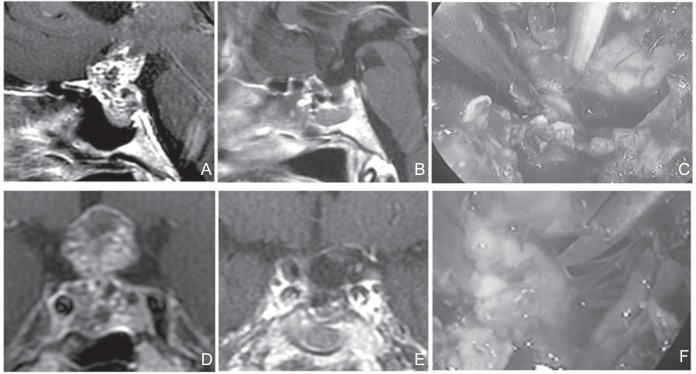
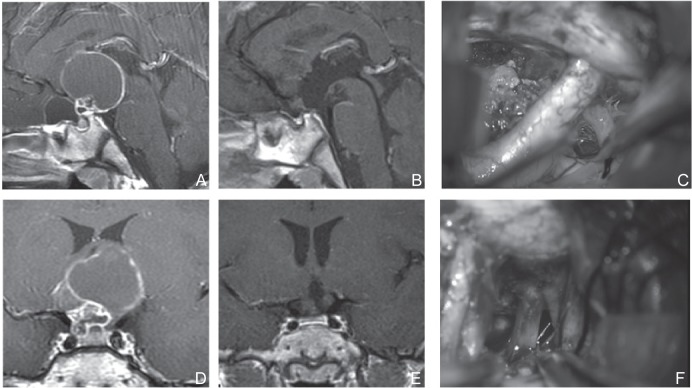
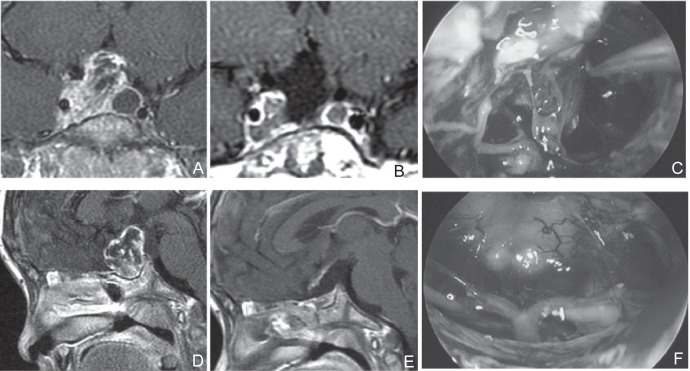
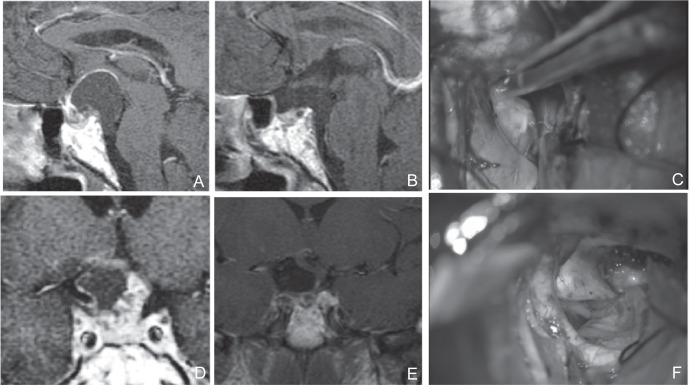
The transsphenoidal approach has been utilized in intrasellar craniopharyngioma surgeries. However, the advent of endoscopic extended transsphenoidal approach (EETSA) has expanded its indication to suprasellar craniopharyngiomas. We compared the indication and limitations of EETSA to those of unilateral basal interhemispheric approach (UBIHA), which presents similar indications for surgery. We analyzed 30 patients with tumors located below the foramen of Monro and the lateral boundary extending slightly beyond the internal carotid artery (UBIHA: N = 18; EETSA: N = 12). Postoperative magnetic resonance imaging (MRI) revealed gross total resection in 10 patients in the EETSA group (83.3%) and 12 in the UBIHA group (66.7%). Postoperative MRI in the EETSA group revealed residual tumor at the cavernous sinus in one patient, at the prepontine in one; in the UBIHA group, residual tumors were located in the retrochiasmatic area in two patients, infundibulum-hypothalamus in one, on the stalk in one, and in the intrasellar region in two. No intergroup differences were observed in the preservation of pituitary function and postoperative improvement of visual function. The extent of resection was better with EETSA than with UBIHA. EETSA is considered the first-line therapy because the distance between the optic chiasm and the superior border of the pituitary is large; the lateral extension does not go beyond the internal carotid artery; and the tumor does not extend inferiorly beyond the posterior clinoid process. However, in patients showing poorly developed sphenoid sinuses or pituitary stalks anterior to the tumor, surgery is difficult regardless of the selection criteria.
经蝶窦入路已用于鞍内颅咽管瘤手术。然而,内镜扩大经蝶窦入路(EETSA)的出现将其适应证扩展至鞍上颅咽管瘤。我们比较了EETSA与单侧基底半球间入路(UBIHA)的适应证及局限性,后者具有相似的手术适应证。我们分析了30例肿瘤位于Monro孔以下且外侧边界略超出颈内动脉的患者(UBIHA组:n = 18;EETSA组:n = 12)。术后磁共振成像(MRI)显示,EETSA组10例患者(83.3%)实现了肿瘤全切,UBIHA组12例患者(66.7%)实现了肿瘤全切。EETSA组术后MRI显示,1例患者海绵窦有残留肿瘤,1例桥前池有残留肿瘤;UBIHA组,2例患者视交叉后区域有残留肿瘤,1例漏斗 - 下丘脑有残留肿瘤,1例肿瘤位于肿瘤蒂部,2例位于鞍内区域。两组在垂体功能保留和视觉功能术后改善方面未观察到组间差异。EETSA的切除范围优于UBIHA。EETSA被认为是一线治疗方法,因为视交叉与垂体上缘之间的距离较大;外侧延伸未超出颈内动脉;且肿瘤向下未延伸至后床突以下。然而,对于蝶窦发育不良或肿瘤前方垂体柄发育不良的患者,无论选择何种标准,手术都很困难。