Menzella Francesco, Lusuardi Mirco, Galeone Carla, Montanari Gloria, Cavazza Alberto, Facciolongo Nicola
Department of Medical Specialties, Pneumology Unit, Arcispedale Santa Maria Nuova-IRCCS, Azienda USL di Reggio Emilia, Via Amendola 2, Viale Risorgimento 56, 42122 Reggio Emilia, Italy.
Unit of Respiratory Rehabilitation, Azienda USL di Reggio Emilia, S. Sebastiano Hospital, Correggio, Italy.
Allergy Asthma Clin Immunol. 2018 Jun 25;14:25. doi: 10.1186/s13223-018-0252-y. eCollection 2018.
Bronchial thermoplasty (BT) is an endoscopic procedure for the treatment of severe refractory asthma, based on the local airways delivery of radio-frequency at 65 °C. Several controlled clinical studies demonstrated the effectiveness of BT on clinical outcomes, particularly the reduction of asthma exacerbations. During procedure or shortly after, significant but transient respiratory adverse events have been reported.
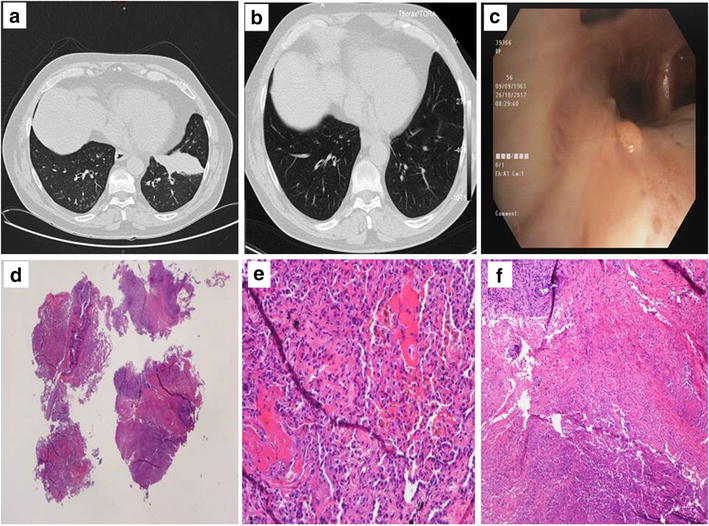
We describe the case of a male, caucasian, 56-year-old, non-smoker patient with non-allergic severe asthma. A few days after the second BT session performed in the left lower lobe, persistent haemoptysis appeared requiring patient hospitalization. A chest CT scan showed mild varicoid bronchiectasis and distal parenchymal infiltrate in the basal anterior segment of the left lower lobe. At fibreoptic bronchoscopy two small nodular neoformations were observed in sub-segmental areas of the same lobe. Histological examination showed mild non-specific inflammation of bronchial mucosa, and some large fragments of peribronchial pulmonary parenchyma with an area of haemorrhagic necrosis. The patient was treated empirically with co-amoxiclav, azithromycin and prednisone. A new chest CT showed a complete resolution of the parenchymal opacity. Finally, the patient underwent the third session of BT, without recurrence of haemoptysis or radiological changes.
Bronchial thermoplasty is a generally safe procedure. To our knowledge this is the first report of necrosis of the treated bronchus and haemoptysis complicating BT after the second session. The pulmonary damage was most likely determined by a thermal shock induced by BT. One hypothesis could be a structural fragility of the treated bronchus, possibly related to bronchiectasis. A technical malfunction of the BT controller or the catheter, causing an excessive energy delivery could not be excluded. Adverse events following BT deserve particular attention but should not discourage clinicians from the application of this promising procedure.
支气管热成形术(BT)是一种用于治疗重度难治性哮喘的内镜手术,通过在65°C下局部气道输送射频能量来实现。多项对照临床研究证明了BT对临床结局的有效性,尤其是减少哮喘发作次数。在手术过程中或术后不久,曾有显著但短暂的呼吸不良事件的报道。
我们描述了一名56岁、非吸烟、白种男性、患有非过敏性重度哮喘的患者。在左下叶进行第二次BT手术后几天,患者出现持续性咯血,需要住院治疗。胸部CT扫描显示左下叶基底前段有轻度静脉曲张样支气管扩张和远端实质浸润。在纤维支气管镜检查中,在同一叶的亚段区域观察到两个小结节状新生物。组织学检查显示支气管黏膜有轻度非特异性炎症,以及一些支气管周围肺实质的大片组织,伴有出血性坏死区域。患者接受了阿莫西林克拉维酸钾、阿奇霉素和泼尼松的经验性治疗。新的胸部CT显示实质模糊影完全消退。最后,患者接受了第三次BT手术,未再出现咯血或影像学改变。
支气管热成形术通常是一种安全的手术。据我们所知,这是首例报道第二次BT手术后出现治疗支气管坏死并伴有咯血的病例。肺部损伤很可能是由BT引起的热休克所致。一种假说可能是治疗支气管的结构脆弱性,可能与支气管扩张有关。不能排除BT控制器或导管的技术故障导致能量输送过多的情况。BT后的不良事件值得特别关注,但不应阻碍临床医生应用这一有前景的手术。