Department of Urology, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan.
Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
World J Surg Oncol. 2018 Jul 9;16(1):135. doi: 10.1186/s12957-018-1411-9.
To clarify if diagnostic ureteroscopy (URS) before radical nephroureterectomy for patients with upper tract urothelial carcinoma (UTUC) will increase the risk of intravesical recurrence.
From retrospective review of cohort at our institution, 502 patients with UTUC who underwent radical nephroureterectomy with bladder cuff excision were enrolled from 1990 to 2013. Cox proportional hazards model was used to analyze the overall survival (OS), disease-free survival (DFS), metastasis-free survival (MFS), and intravesical recurrence-free survival (IVRFS). The log-rank test was used for comparing survival curves. All potential risk factors were included in the multivariate Cox proportional hazards model to recognize independent predictors. From NHI database, we included patients of UTUC without bladder cancer history using population-based database in Taiwan from 1996 to 2013. In total, 3079 URS and 2634 non-URS patients with UTUC were identified. Univariate and multivariate Cox proportional hazards regressions were performed to measure the risk of IVRFS and all-cause mortality.
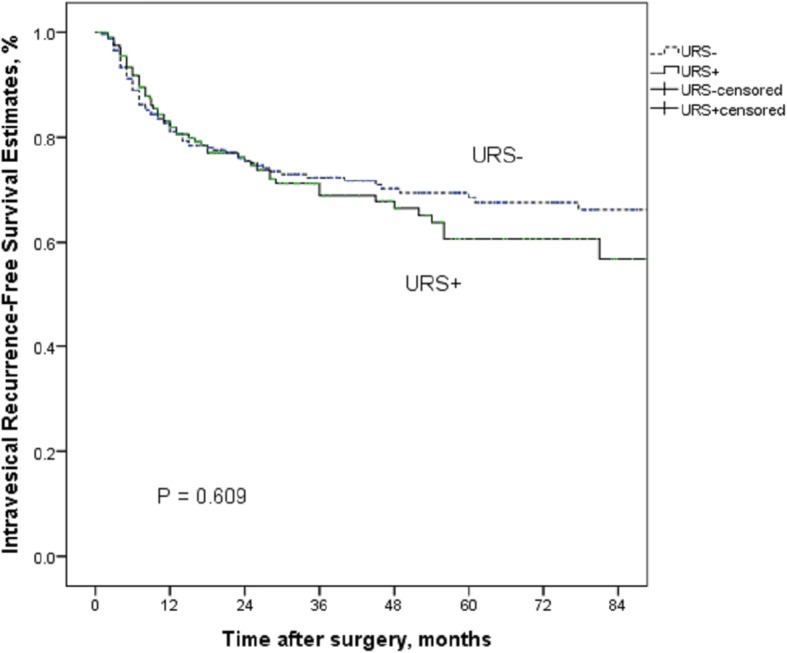
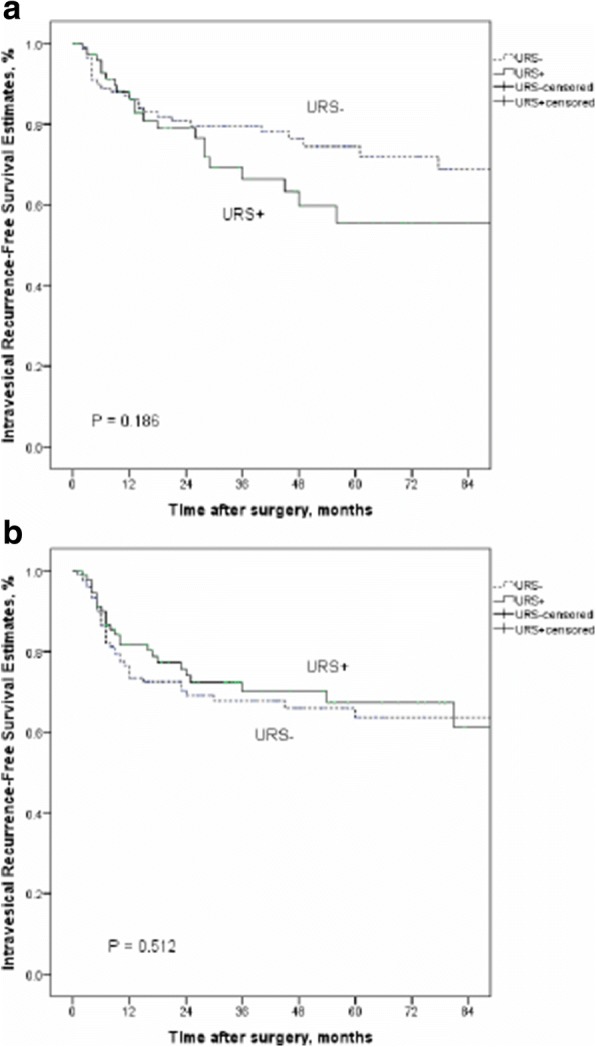
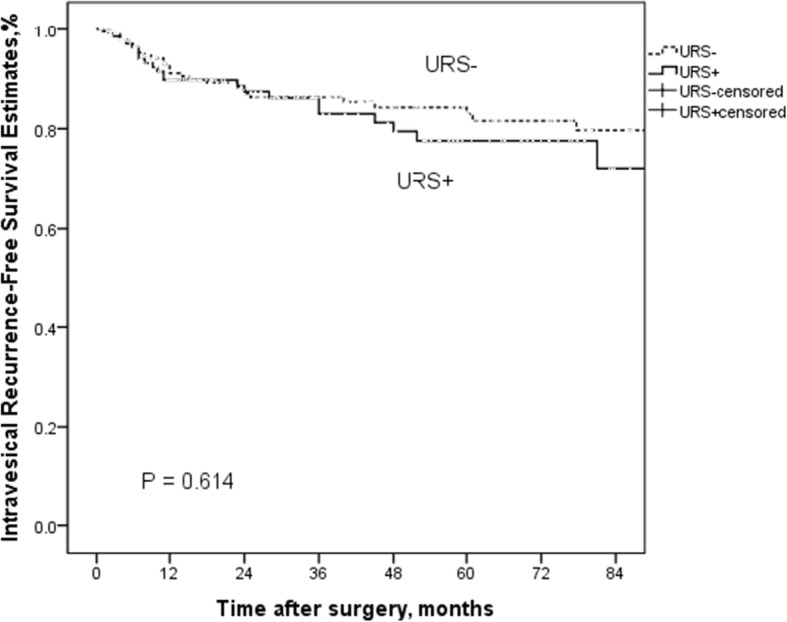
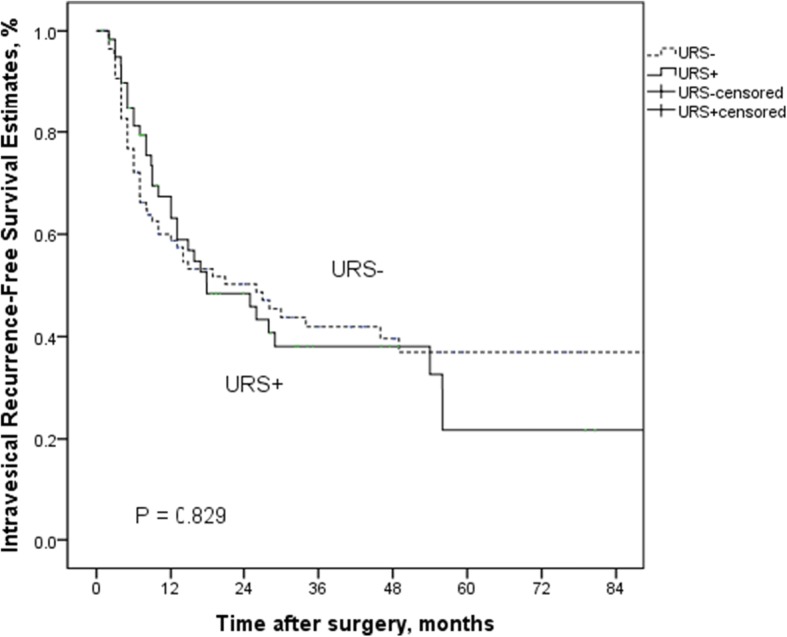
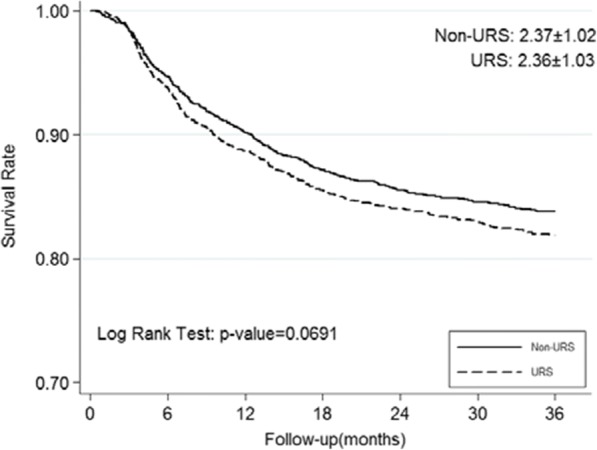
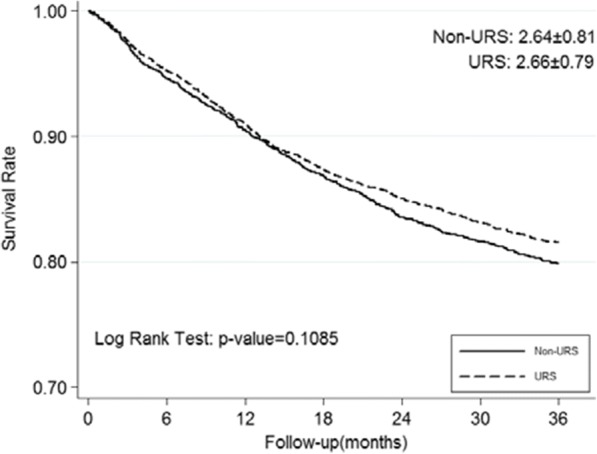
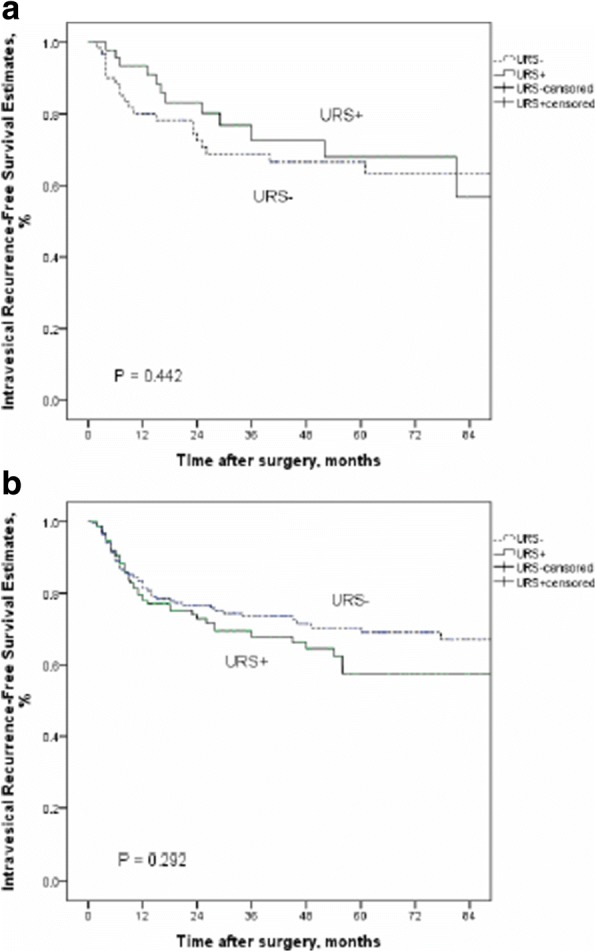
From our database, the comparison of clinicopathological characteristics in UTUC patients between with URS biopsy group (URS+) (n = 206, 41%) and without URS biopsy group (URS-) (n = 296, 59%) was insignificantly different excluding surgical method. URS biopsy is not associated with worse OS (p = 0.720), DFS (p = 0.294), MFS (p = 0.808), and IVRFS (p = 0.560) by multivariate analysis. Only bladder cancer history is an independent significant factor to predict IVR (p < 0.001). The same result from NHI database, URS before radical surgery will not increase the risk of IVRFS [adjusted HR 1.136, 95% CI 1.00-1.30; P = 0.059] and OS [adjusted HR 0.919, 95% CI 0.82-1.04; P = 0.164].
Preoperative URS manipulation is not associated with higher risk of IVRFS even in patients without bladder cancer history. Diagnostic URS is feasible to compensate the insufficient information of image in patients with UTUC.
为明确诊断性输尿管镜检查(URS)在上尿路尿路上皮癌(UTUC)患者根治性肾输尿管切除术前是否会增加膀胱内复发的风险。
本研究通过对我院队列的回顾性分析,纳入了 1990 年至 2013 年间接受根治性肾输尿管切除术加膀胱袖套切除的 502 例 UTUC 患者。采用 Cox 比例风险模型分析总生存(OS)、无病生存(DFS)、无转移生存(MFS)和膀胱内无复发生存(IVRFS)。对数秩检验用于比较生存曲线。将所有潜在的危险因素纳入多变量 Cox 比例风险模型,以识别独立的预测因素。我们从国民健康保险数据库中纳入了台湾地区 1996 年至 2013 年无膀胱癌病史的 UTUC 患者,共纳入 3079 例接受 URS 和 2634 例未接受 URS 的 UTUC 患者。采用单因素和多因素 Cox 比例风险回归分析测量 IVRFS 和全因死亡率的风险。
在我们的数据库中,与未接受 URS 活检组(URS-)(n=296,59%)相比,接受 URS 活检组(URS+)(n=206,41%)的 UTUC 患者的临床病理特征比较无显著差异,除外手术方式。多因素分析显示,URS 活检与较差的 OS(p=0.720)、DFS(p=0.294)、MFS(p=0.808)和 IVRFS(p=0.560)无关。只有膀胱癌病史是预测 IVR 的独立显著因素(p<0.001)。从 NHIRD 数据库中得到的相同结果是,根治性手术前的 URS 不会增加 IVRFS 的风险[调整后的 HR 1.136,95%CI 1.00-1.30;P=0.059]和 OS[调整后的 HR 0.919,95%CI 0.82-1.04;P=0.164]。
即使在无膀胱癌病史的患者中,术前 URS 操作也与较高的 IVRFS 风险无关。诊断性 URS 可在 UTUC 患者中弥补影像学信息不足的问题。