Service d'Anesthésie Réanimation Chirurgicale, Hôpitaux Universitaires, Strasbourg, France.
Institut Hospitalo-Universitaire de Strasbourg, Strasbourg, France.
PLoS One. 2018 Jul 11;13(7):e0199369. doi: 10.1371/journal.pone.0199369. eCollection 2018.
Maintaining normothermia during anesthesia is imperative to provide quality patient care and to prevent adverse outcomes. Prolonged laparoscopic procedures have been identified as a potential risk factor for hypothermia, due to continuous insufflation of cold and dry carbon dioxide. Perioperative hypothermia is associated with increased hospital cost and many complications including; impaired drug metabolism, impaired immune function, cardiac morbidity, shivering, coagulopathy.
In this experimental study, four pigs underwent four interventions each, resulting in 16 total trials. Using standardized general anesthesia in a randomized Latin-square sequence the four interventions include: 1. Control group without an administered pneumoperitoneum, 2. Administered standard pneumoperitoneum using 21°C insufflated gas and under-body forced-air warming, 3. Administered pneumoperitoneum with insufflation of warmed/humidified carbon dioxide, 4. Administered pneumoperitoneum with insufflation of warmed/humidified carbon dioxide and under-body forced-air warming. The primary outcome was distal esophageal temperature change 4 hours after trocar insertion.
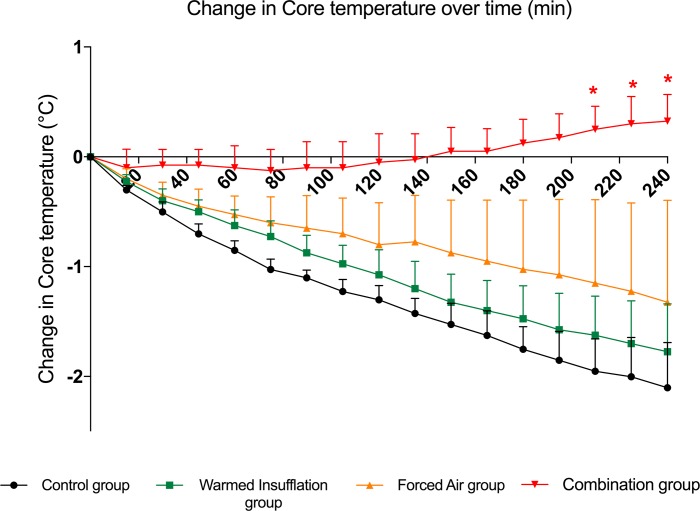
Four hours after trocar insertion, pigs in the control group lost 2.1 ± 0.4°C; pigs with warmed and humidified insufflation lost 1.8 ± 0.4°C; pigs with forced-air warming group lost 1.3 ± 0.9°C; and pigs exposed to a combination of warmed and humidified insufflation with forced-air warming increased by 0.3 ± 0.2°C.
This experimental animal study provides evidence that a combination of warmed and humidified insufflation of carbon dioxide (CO2) in conjunction with forced-air warming is an effective strategy in the prevention of perioperative hypothermia. Further clinical trials investigating humans are therefore indicated.
在麻醉期间保持正常体温对于提供高质量的患者护理和预防不良后果至关重要。由于持续注入冷而干燥的二氧化碳,长时间的腹腔镜手术已被确定为导致体温过低的潜在危险因素。围手术期低体温与增加医院成本和许多并发症相关,包括:药物代谢受损、免疫功能受损、心脏发病率、寒战、凝血功能障碍。
在这项实验研究中,四只猪接受了每种干预措施各四次,总共进行了 16 次试验。使用标准化全身麻醉并以随机拉丁方序列进行,四种干预措施包括:1. 未进行气腹的对照组,2. 采用 21°C 注入气体和下半身强制空气加热的标准气腹,3. 注入温热/加湿二氧化碳的气腹,4. 注入温热/加湿二氧化碳并进行下半身强制空气加热的气腹。主要结局是套管插入后 4 小时远端食管温度变化。
套管插入后 4 小时,对照组的猪体温下降了 2.1 ± 0.4°C;接受温热加湿注入的猪体温下降了 1.8 ± 0.4°C;接受强制空气加热的猪体温下降了 1.3 ± 0.9°C;接受温热加湿注入和强制空气加热的组合的猪体温升高了 0.3 ± 0.2°C。
这项实验动物研究提供了证据,表明温热加湿的二氧化碳(CO2)注入与强制空气加热相结合是预防围手术期低体温的有效策略。因此,需要进一步进行人类临床试验。