Acquired Immunodeficiency Research Center, Isfahan University of Medical Science, Isfahan, Iran.
Center for Chronic Immunodeficiency, University Hospital, Freiburg, Germany.
BMC Pregnancy Childbirth. 2018 Jul 11;18(1):299. doi: 10.1186/s12884-018-1927-6.
Patients with primary immunodeficiency disease (PID) who survive to adulthood and willing to have a child mostly are worried whether their disease affects their fertility and/or pregnancy and also if their child would be predisposed to PID.
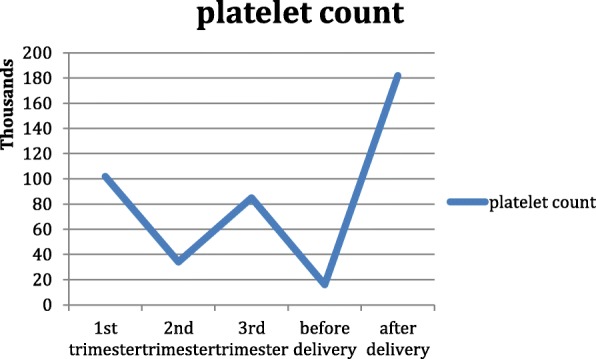
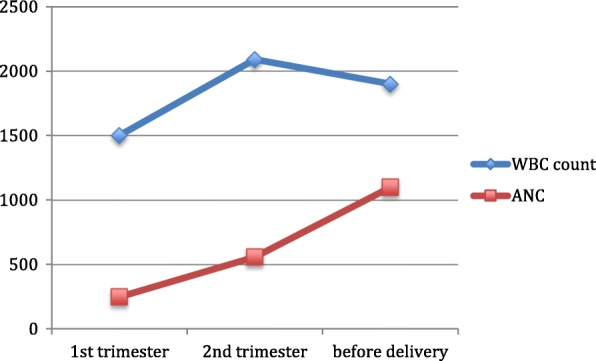
We report the outcome of conception, pregnancy and their management in 9 families with definite diagnosis of PID. A chronic granulomatous disease subject with an uneventful pregnancy developed fungal sacral osteomyelitis few weeks after delivery. A pregnant common variable immunodeficiency disease (CVID) patient with idiopathic thrombocytopenia had platelet count dropped before delivery. A sever neutropenic mother who refused to get IFNγ delivered two healthy children. A CVID case intolerant to IVIg with eclampsia and PTE delivered a baby. Another CVID female gave birth to a baby without being on any treatment since she was not diagnosed with immunodeficiency disease at that time. A healthy girl was implanted via preimplantation gender selection in a family who owned a Wiskott Aldrich-affected son. A family who had two children with Ataxia Telangiectasia used donated oocyte for their 3rd child. Prenatal genetic diagnosis was used to screen the fetus for the impaired BTK and CVID genes detected in sibling and father respectively in 2 separate families.
Pregnancy in PID patients is more complex than normal population. Because, not only it has the chance of being inherited by the offspring, but also there are some risks for the mother if she has any kind of immunity component defects. So consultation with a clinical geneticist is crucial to choose the best available approach. They also should be observed and followed by a clinical immunologist to take the best possible safe care.
患有原发性免疫缺陷病(PID)并存活至成年且愿意生育的患者大多担心他们的疾病是否会影响他们的生育能力和/或妊娠,以及他们的孩子是否易患 PID。
我们报告了 9 个 PID 明确诊断的家庭的受孕、妊娠及其管理结果。一名患有慢性肉芽肿病的患者,妊娠期间无并发症,分娩后数周出现真菌性骶骨骨髓炎。一名患有特发性血小板减少性紫癜的妊娠普通可变免疫缺陷病(CVID)患者,在分娩前血小板计数下降。一名拒绝接受 IFNγ治疗的严重中性粒细胞减少症母亲,成功分娩了两名健康的孩子。一名不能耐受 IVIg 的 CVID 患者出现子痫和 PTE,分娩了一个婴儿。另一名 CVID 女性在未被诊断为免疫缺陷病时怀孕,未接受任何治疗就分娩了一个婴儿。一个健康的女孩通过植入前性别选择在一个患有威斯科特-奥尔德里奇综合征(Wiskott Aldrich syndrome)儿子的家庭中受孕。一个有两个患有共济失调毛细血管扩张症(ataxia telangiectasia)的孩子的家庭,使用捐赠的卵子来孕育他们的第三个孩子。两个家庭分别对胎儿进行了产前基因诊断,以筛查同胞和父亲分别携带的异常 BTK 和 CVID 基因。
PID 患者的妊娠比正常人群更为复杂。因为,它不仅有机会遗传给后代,而且如果母亲有任何免疫成分缺陷,也会对母亲造成一些风险。因此,咨询临床遗传学家对于选择最佳可行方法至关重要。他们还应该由临床免疫学家进行观察和随访,以获得最佳的安全护理。