1Center for Clinical Evidence Synthesis, Tufts Medical Center, 800 Washington Street, Box 63, Boston, MA 02111 USA.
2Merck & Co., Inc., Kenilworth, NJ USA.
Antimicrob Resist Infect Control. 2018 Jul 4;7:79. doi: 10.1186/s13756-018-0370-9. eCollection 2018.
Identifying risk factors predicting acquisition of resistant will aid surveillance and diagnostic initiatives and can be crucial in early and appropriate antibiotic therapy. We conducted a systematic review examining risk factors of acquisition of resistant among hospitalized patients.
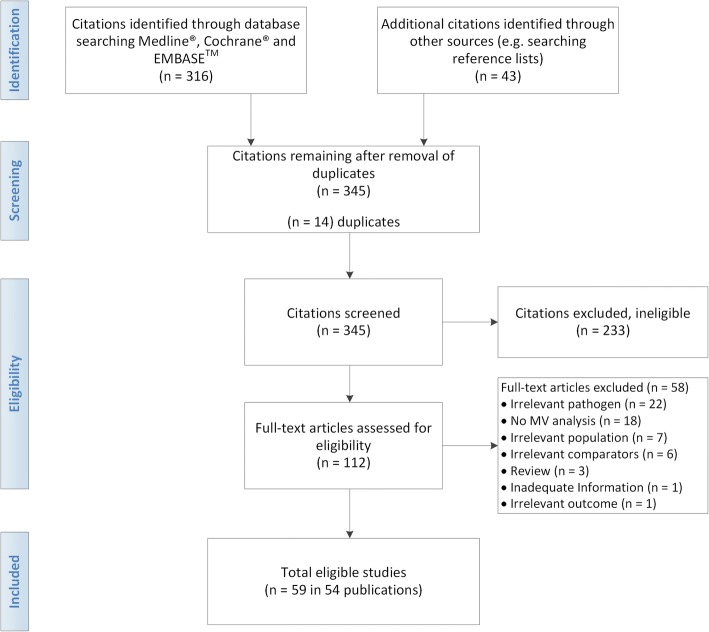
MEDLINE®, EMBASE®, and Cochrane Central were searched between 2000 and 2016 for studies examining independent risk factors associated with acquisition of resistant , among hospitalized patients. Random effects model meta-analysis was conducted when at least three or more studies were sufficiently similar.
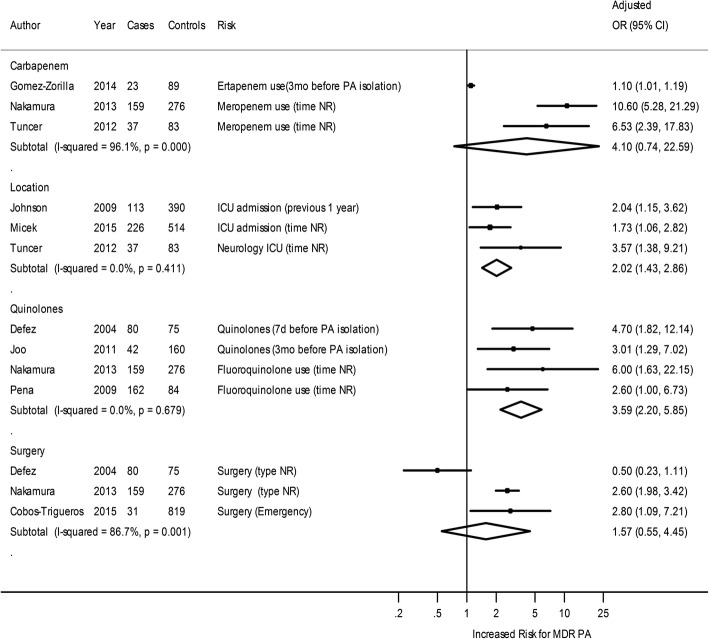
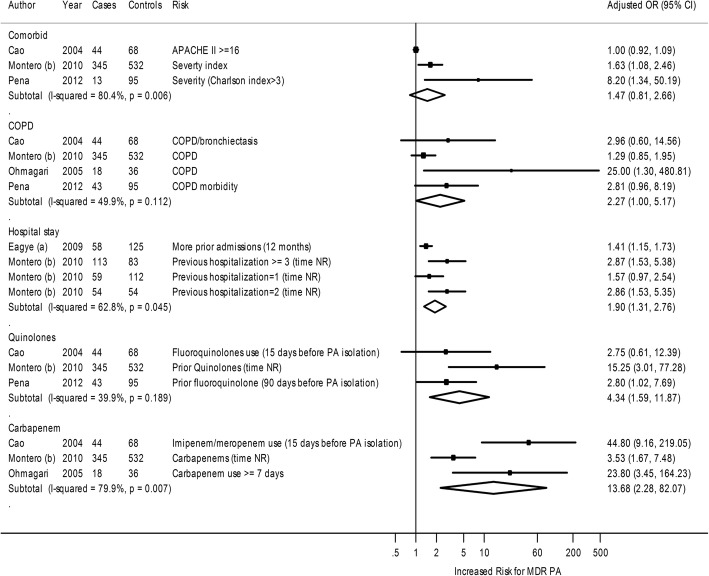
Of the 54 eligible articles, 28 publications (31studies) examined multi-drug resistant (MDR) or extensively drug resistant (XDR) and 26 publications (29 studies) examined resistant The acquisition of MDR , as compared with non-MDR , was significantly associated with intensive care unit (ICU) admission (3 studies: summary adjusted odds ratio [OR] 2.2) or use of quinolones (4 studies: summary adjusted OR 3.59). Acquisition of MDR or XDR compared with susceptible was significantly associated with prior hospital stay (4 studies: summary adjusted OR 1.90), use of quinolones (3 studies: summary adjusted OR 4.34), or use of carbapenems (3 studies: summary adjusted OR 13.68). The acquisition of MDR compared with non- was significantly associated with prior use of cephalosporins (3 studies: summary adjusted OR 3.96), quinolones (4 studies: summary adjusted OR 2.96), carbapenems (6 studies: summary adjusted OR 2.61), and prior hospital stay (4 studies: summary adjusted OR 1.74). The acquisition of carbapenem-resistant compared with susceptible , was statistically significantly associated with prior use of piperacillin-tazobactam (3 studies: summary adjusted OR 2.64), vancomycin (3 studies: summary adjusted OR 1.76), and carbapenems (7 studies: summary adjusted OR 4.36).
Prior use of antibiotics and prior hospital or ICU stay was the most significant risk factors for acquisition of resistant . These findings provide guidance in identifying patients that may be at an elevated risk for a resistant infection and emphasize the importance of antimicrobial stewardship and infection control in hospitals.
识别预测耐药菌获得的风险因素有助于监测和诊断计划,并且在早期和适当的抗生素治疗中至关重要。我们进行了一项系统评价,研究了住院患者获得耐药菌的风险因素。
2000 年至 2016 年期间,我们在 MEDLINE®、EMBASE®和 Cochrane Central 中搜索了研究住院患者获得耐药菌的独立风险因素的研究。当至少有三个或更多研究足够相似时,进行了随机效应模型荟萃分析。
在 54 篇合格的文章中,28 篇出版物(31 项研究)研究了多药耐药(MDR)或广泛耐药(XDR),26 篇出版物(29 项研究)研究了耐药菌。与非 MDR 相比,MDR 的获得与重症监护病房(ICU)入院(3 项研究:汇总调整后的优势比[OR]2.2)或使用喹诺酮类药物(4 项研究:汇总调整后的 OR 3.59)显著相关。与敏感菌相比,MDR 或 XDR 的获得与既往住院史(4 项研究:汇总调整后的 OR 1.90)、使用喹诺酮类药物(3 项研究:汇总调整后的 OR 4.34)或使用碳青霉烯类药物(3 项研究:汇总调整后的 OR 13.68)显著相关。与非 MDR 相比,MDR 的获得与头孢菌素(3 项研究:汇总调整后的 OR 3.96)、喹诺酮类药物(4 项研究:汇总调整后的 OR 2.96)、碳青霉烯类药物(6 项研究:汇总调整后的 OR 2.61)和既往住院史(4 项研究:汇总调整后的 OR 1.74)的使用显著相关。与敏感菌相比,耐碳青霉烯类药物的获得与哌拉西林他唑巴坦(3 项研究:汇总调整后的 OR 2.64)、万古霉素(3 项研究:汇总调整后的 OR 1.76)和碳青霉烯类药物(7 项研究:汇总调整后的 OR 4.36)的使用显著相关。
既往使用抗生素和既往住院或 ICU 住院是获得耐药菌的最重要危险因素。这些发现为识别可能处于耐药感染风险增加的患者提供了指导,并强调了医院内抗菌药物管理和感染控制的重要性。