Departments of Epidemiology and.
Medicine, Johns Hopkins University, Baltimore, Maryland.
Clin J Am Soc Nephrol. 2018 Aug 7;13(8):1144-1152. doi: 10.2215/CJN.13811217. Epub 2018 Jul 12.
All randomized trials of direct oral anticoagulants in atrial fibrillation excluded patients with severe kidney disease. The safety and effectiveness of direct oral anticoagulants across the range of eGFR in real-world settings is unknown. Our objective is to quantify the risk of bleeding and benefit of ischemic stroke prevention for direct oral anticoagulants compared with warfarin in patients with atrial fibrillation with and without CKD.
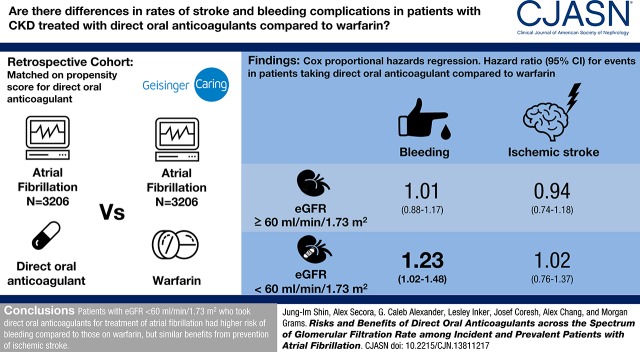
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We created a propensity score-matched cohort of 3206 patients with atrial fibrillation and direct oral anticoagulant use and 3206 patients with atrial fibrillation using warfarin from October of 2010 to February of 2017 in an electronic health record (Geisinger Health System). The risks of bleeding and ischemic stroke were compared between direct oral anticoagulant and warfarin users using Cox proportional hazards regression, stratified by eGFR (≥60 and <60 ml/min per 1.73 m).
The mean (SD) age of the 6412 participants was 72 (12) years, 47% were women, and average eGFR was 69 (21) ml/min per 1.73 m. There were 1181 bleeding events and 466 ischemic strokes over 7391 person-years of follow-up. Compared with warfarin use, the hazard ratios (HRs) (95% confidence interval [95% CI]) of bleeding associated with direct oral anticoagulant use were 1.01 (0.88 to 1.17) and 1.23 (1.02 to 1.48) for those with eGFR≥60 and eGFR<60 ml/min per 1.73 m, respectively (-interaction=0.10). There was no difference between direct oral anticoagulant and warfarin users in the risk of ischemic stroke: HRs (95% CI) of 0.94 (0.74 to 1.18) and 1.02 (0.76 to 1.37) for those with eGFR≥60 and eGFR<60 ml/min per 1.73 m, respectively (-interaction=0.70). Similar findings were observed with individual drugs.
In a large health care system, patients with eGFR<60 ml/min per 1.73 m who took direct oral anticoagulants for atrial fibrillation had slightly higher risk of bleeding compared with those on warfarin, but similar benefits from prevention of ischemic stroke.
所有房颤患者的直接口服抗凝剂随机试验均排除了严重肾脏疾病患者。在真实环境中,直接口服抗凝剂在整个 eGFR 范围内的安全性和有效性尚不清楚。我们的目的是定量评估房颤患者中直接口服抗凝剂与华法林相比,在伴有和不伴有 CKD 时的出血风险和预防缺血性卒中的获益。
设计、环境、参与者和测量方法:我们创建了一个从 2010 年 10 月至 2017 年 2 月在电子健康记录(Geisinger 健康系统)中使用直接口服抗凝剂和华法林的 3206 例房颤患者的倾向评分匹配队列。使用 Cox 比例风险回归,按 eGFR(≥60 和 <60 ml/min/1.73 m)分层,比较直接口服抗凝剂和华法林使用者的出血风险和缺血性卒中风险。
6412 名参与者的平均(标准差)年龄为 72(12)岁,47%为女性,平均 eGFR 为 69(21)ml/min/1.73 m。在 7391 人年的随访中,共发生 1181 例出血事件和 466 例缺血性卒中。与华法林相比,eGFR≥60 和 eGFR<60 ml/min/1.73 m 的直接口服抗凝剂使用者的出血风险 HR(95%CI)分别为 1.01(0.88 至 1.17)和 1.23(1.02 至 1.48)(-交互作用=0.10)。eGFR≥60 和 eGFR<60 ml/min/1.73 m 的直接口服抗凝剂使用者和华法林使用者的缺血性卒中风险无差异:HR(95%CI)分别为 0.94(0.74 至 1.18)和 1.02(0.76 至 1.37)(-交互作用=0.70)。对于个体药物也观察到类似的结果。
在大型医疗保健系统中,eGFR<60 ml/min/1.73 m 的房颤患者使用直接口服抗凝剂的出血风险略高于华法林,但预防缺血性卒中的获益相似。