Giustini Nicholas, Bernthal Nicholas M, Bukata Susan V, Singh Arun S
1Division of Hematology and Oncology, University of California Los Angeles (UCLA), 2825 Santa Monica Blvd. Suite 200, Santa Monica, CA 90404 USA.
2Division of Orthopedic Oncology, University of California Los Angeles (UCLA), 1250 16th Street, Suite 2100, Santa Monica, CA 90404 USA.
Clin Sarcoma Res. 2018 Jul 10;8:14. doi: 10.1186/s13569-018-0101-2. eCollection 2018.
Tenosynovial giant cell tumors (TGCTs) or giant cell tumors of tendon sheath are neoplasms that arise in the synovium. They can be categorized as nodular (localized) or diffuse type (D-TGCT). Historically, surgery has been the mainstay of therapy, but diffuse type disease recurs at a high rate and treatment often requires increasingly morbid procedures. Elucidation of the importance of the colony-stimulating factor (CSF1)/CSF1 receptor (CSF1R) pathway in the pathogenesis of this disease has created significant interest in targeting this pathway as a novel TGCT treatment approach. Pexidartinib, a selective tyrosine kinase inhibitor against CSF1R, showed an 83% disease control rate (52% with partial response and 31% with stable disease) in a recent phase 1 study of patients with TGCT.
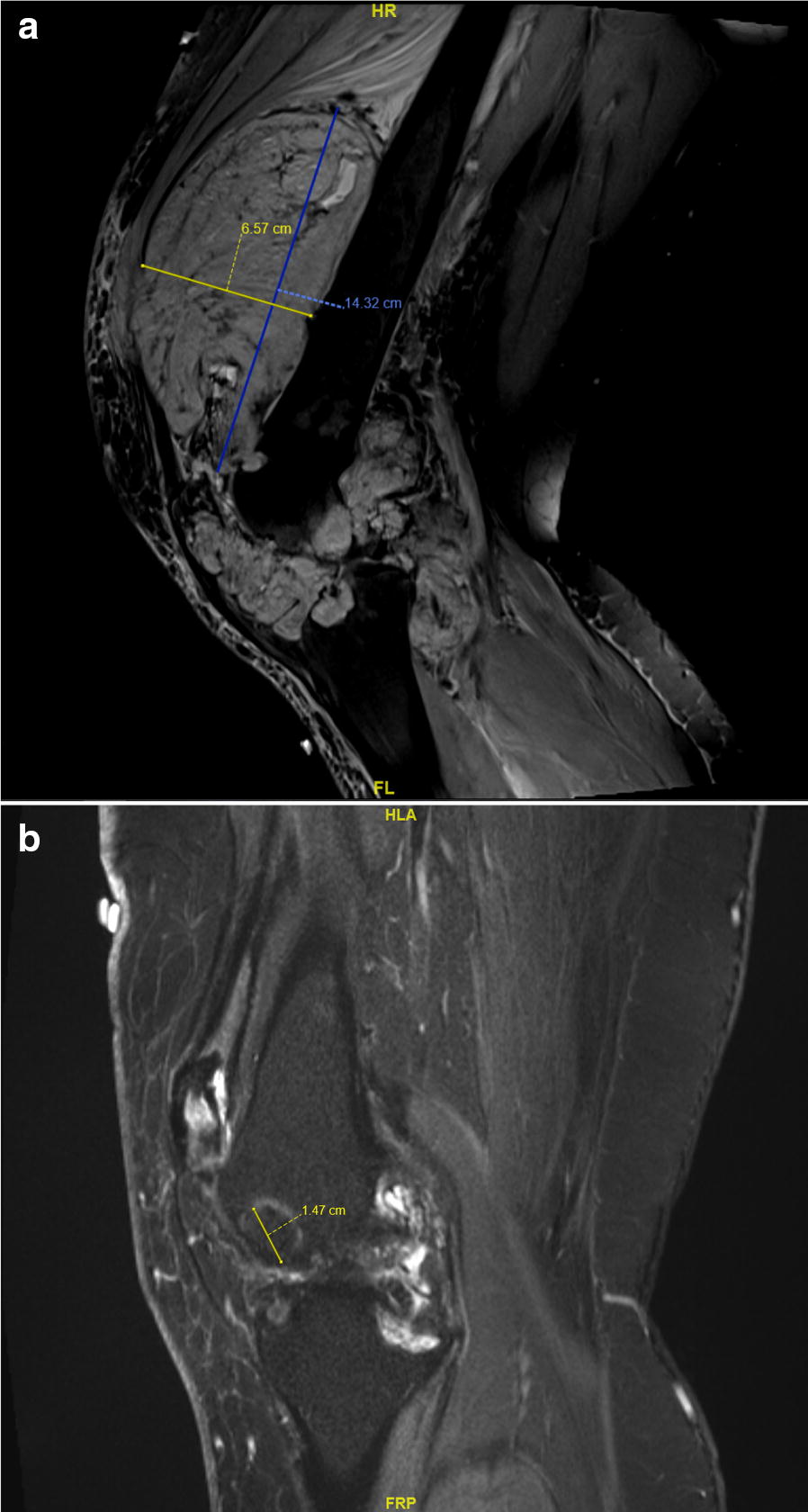
We present an illustrative example of a TGCT patient who would have required a morbid operation who derived considerable clinical benefit from pexidartinib treatment. Her tumor volume decreased by 48% after 4 months of treatment, and 55 months after starting treatment the patient exhibits continued disease stability with minimal clinical symptoms, and significant improvement in functional status.
This case illustrates the effectiveness of systemic therapy in controlling a disease associated with high surgical morbidity. This approach may be especially useful in the treatment of extra-articular disease which often invades neurovascular bundles; as the effectiveness in metastatic disease is still unknown. In the future, systemic treatment for TGCT may be appropriate for the neoadjuvant setting to decrease disease burden prior to surgery with the aim of decreasing recurrence rates. However, properly designed prospective studies will need to be carried out to answer these questions.
腱鞘巨细胞瘤(TGCTs)或腱鞘巨细胞瘤是起源于滑膜的肿瘤。它们可分为结节型(局限性)或弥漫型(D-TGCT)。从历史上看,手术一直是主要的治疗方法,但弥漫型疾病复发率很高,治疗往往需要越来越复杂的手术。阐明集落刺激因子(CSF1)/CSF1受体(CSF1R)途径在该疾病发病机制中的重要性,引发了人们对将该途径作为一种新型TGCT治疗方法的极大兴趣。培西达替尼是一种针对CSF1R的选择性酪氨酸激酶抑制剂,在最近一项针对TGCT患者的1期研究中显示出83%的疾病控制率(52%部分缓解,31%病情稳定)。
我们展示了一个TGCT患者的典型例子,该患者原本需要进行复杂手术,而培西达替尼治疗使其获得了显著的临床益处。治疗4个月后,她的肿瘤体积减少了48%,开始治疗55个月后,患者病情持续稳定,临床症状轻微,功能状态有显著改善。
该病例说明了全身治疗在控制一种手术并发症高的疾病方面的有效性。这种方法在治疗经常侵犯神经血管束的关节外疾病时可能特别有用;因为其对转移性疾病的有效性仍未知。未来,TGCT的全身治疗可能适用于新辅助治疗,以在手术前减轻疾病负担,从而降低复发率。然而,需要进行设计合理的前瞻性研究来回答这些问题。