Department of Emergency Medicine, Yeouido St. Mary's Hospital, The Catholic University of Korea, College of Medicine, 10, 63-ro, Yeongdeungpo-gu, Seoul, 07345, Republic of Korea.
Scand J Trauma Resusc Emerg Med. 2018 Jul 13;26(1):59. doi: 10.1186/s13049-018-0529-7.
Outcome prediction is crucial for out-of-hospital cardiac arrest (OHCA) survivors. Several attempts have been made to use the bispectral index (BIS) for this purpose. We aimed to investigate the prognostic power of the BIS during the early stage of targeted temperature management (TTM) after OHCA.
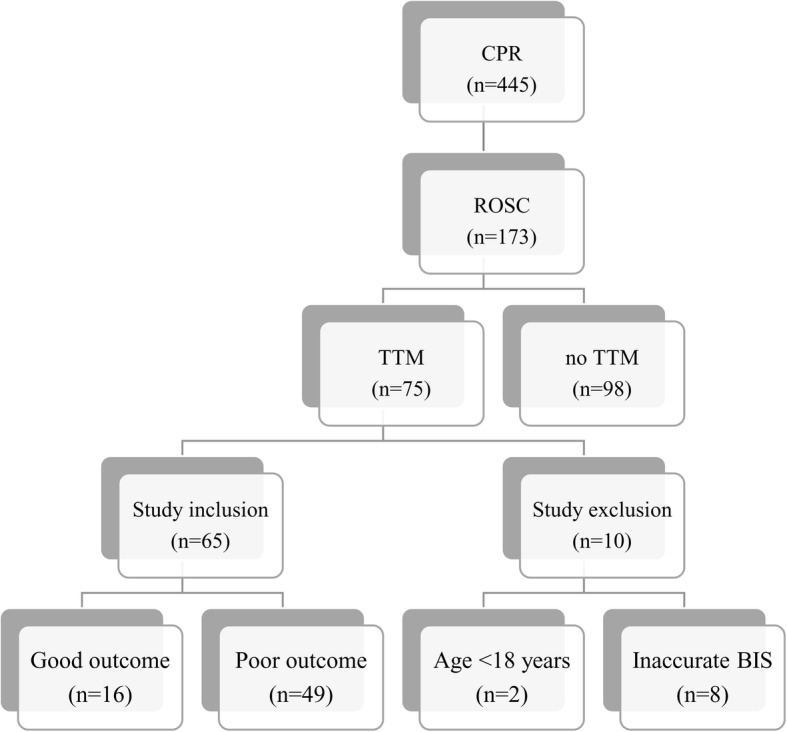
From Jan 2014 to Feb 2017, the BIS was determined in OHCA patients as soon as possible after the start of TTM. We injected a neuro-muscular blocking agent and recoded the BIS value and the time when the electromyographic (EMG) factor reached zero. The primary outcome was the cerebral performance category scale (CPC) score at 6 months, and a poor outcome was defined as a CPC score of 3, 4, or 5. The exclusion criteria were age under 18 years, traumatic cardiac arrest, and BIS data with a non-zero EMG factor.
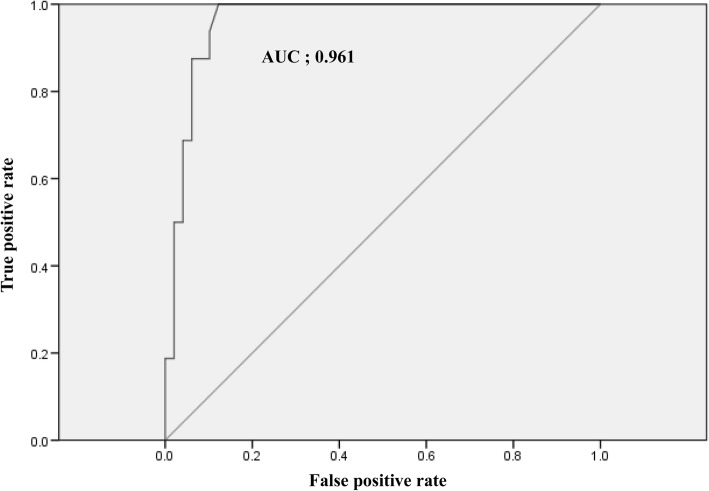
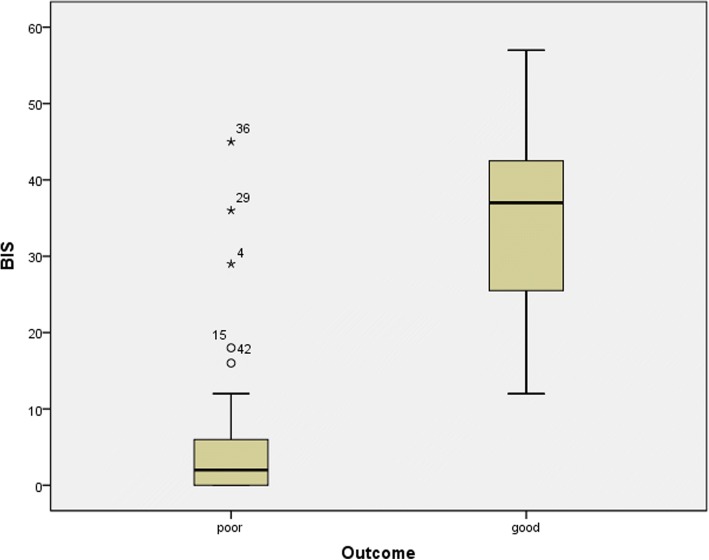
Sixty-five patients were included in this study. Good outcomes were observed for 16 patients (24.6%), and poor outcomes were observed for 49 patients (75.4%). The mean time of BIS recording was 2.3 ± 1.0 h after return of spontaneous circulation (ROSC). The mean BIS values of the good outcome and poor outcome groups were 35.6 ± 13.1 and 5.5 ± 9.2, respectively (p < 0.001). The area under the curve was 0.961. Use of a cut-off value of 20.5 to predict a good outcome yielded a sensitivity of 87.5% and specificity of 93.9%. Use of a cut-off value of 10.5 to predict a poor outcome yielded a sensitivity of 87.8% and specificity of 100%.
With the help of BIS, physicians could predict that a patient who has BIS value over 20.5 after ROSC could have a big chance to get good neurological outcome in less than three hours.
对于院外心脏骤停(OHCA)幸存者,预后预测至关重要。已经尝试了多种方法来使用双频谱指数(BIS)进行此目的。我们旨在研究 OHCA 后靶向体温管理(TTM)早期阶段 BIS 的预后能力。
从 2014 年 1 月至 2017 年 2 月,在 TTM 开始后尽快在 OHCA 患者中确定 BIS。我们注射了神经肌肉阻滞剂,并记录 BIS 值和肌电图(EMG)因子达到零时的时间。主要结局是 6 个月时的脑功能分类量表(CPC)评分,预后不良定义为 CPC 评分为 3、4 或 5。排除标准为年龄<18 岁,创伤性心脏骤停和 BIS 数据的 EMG 因子不为零。
本研究共纳入 65 例患者。16 例(24.6%)患者预后良好,49 例(75.4%)患者预后不良。ROSC 后记录 BIS 的平均时间为 2.3±1.0 h。预后良好和预后不良组的平均 BIS 值分别为 35.6±13.1 和 5.5±9.2(p<0.001)。曲线下面积为 0.961。使用 20.5 的截断值预测良好预后的敏感性为 87.5%,特异性为 93.9%。使用 10.5 的截断值预测不良预后的敏感性为 87.8%,特异性为 100%。
借助 BIS,医生可以预测在 ROSC 后 BIS 值超过 20.5 的患者在不到 3 小时内获得良好神经预后的可能性较大。