Department of Intensive Care, Emergency Medicine and Anaesthesiology, Fondazione Policlinico Universitario "Agostino Gemelli"-IRCCS, Largo Francesco Vito, 1, 00168, Rome, Italy.
Institute of Anaesthesiology and Intensive Care Medicine, Università Cattolica del Sacro Cuore, Rome, Italy.
Intensive Care Med. 2022 Apr;48(4):389-413. doi: 10.1007/s00134-022-06618-z. Epub 2022 Mar 4.
To assess the ability of clinical examination, blood biomarkers, electrophysiology or neuroimaging assessed within 7 days from return of spontaneous circulation (ROSC) to predict good neurological outcome, defined as no, mild, or moderate disability (CPC 1-2 or mRS 0-3) at discharge from intensive care unit or later, in comatose adult survivors from cardiac arrest (CA).
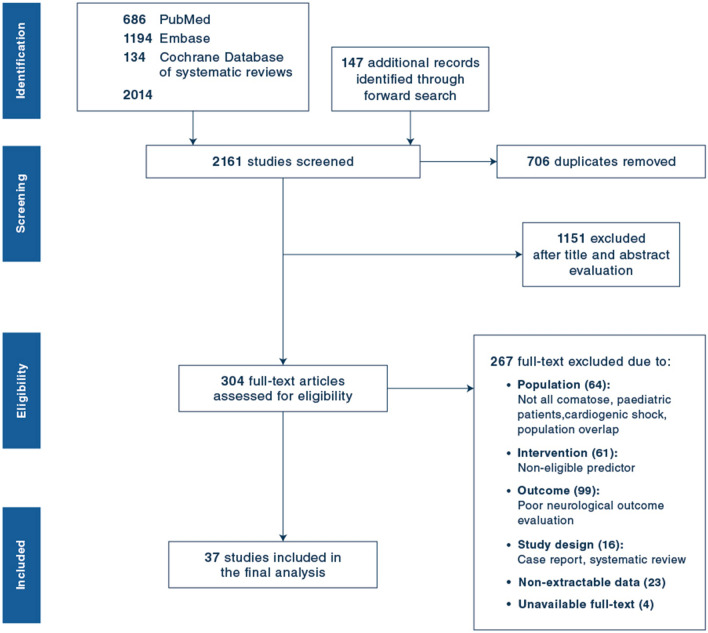
PubMed, EMBASE, Web of Science and the Cochrane Database of Systematic Reviews were searched. Sensitivity and specificity for good outcome were calculated for each predictor. The risk of bias was assessed using the QUIPS tool.
A total of 37 studies were included. Due to heterogeneities in recording times, predictor thresholds, and definition of some predictors, meta-analysis was not performed. A withdrawal or localisation motor response to pain immediately or at 72-96 h after ROSC, normal blood values of neuron-specific enolase (NSE) at 24 h-72 h after ROSC, a short-latency somatosensory evoked potentials (SSEPs) N20 wave amplitude > 4 µV or a continuous background without discharges on electroencephalogram (EEG) within 72 h from ROSC, and absent diffusion restriction in the cortex or deep grey matter on MRI on days 2-7 after ROSC predicted good neurological outcome with more than 80% specificity and a sensitivity above 40% in most studies. Most studies had moderate or high risk of bias.
In comatose cardiac arrest survivors, clinical, biomarker, electrophysiology, and imaging studies identified patients destined to a good neurological outcome with high specificity within the first week after cardiac arrest (CA).
评估临床检查、血液生物标志物、电生理学或神经影像学在自主循环恢复(ROSC)后 7 天内评估的能力,以预测昏迷的心脏骤停(CA)成年幸存者在从重症监护病房出院或之后的良好神经结局,定义为无、轻度或中度残疾(CPC 1-2 或 mRS 0-3)。
检索了 PubMed、EMBASE、Web of Science 和 Cochrane 系统评价数据库。为每个预测因子计算了良好结局的敏感性和特异性。使用 QUIPS 工具评估偏倚风险。
共纳入 37 项研究。由于记录时间、预测因子阈值和某些预测因子的定义存在异质性,因此未进行荟萃分析。ROSC 后立即或 72-96 小时后对疼痛有撤回或定位运动反应,ROSC 后 24-72 小时内神经元特异性烯醇化酶(NSE)的正常血液值,短潜伏期体感诱发电位(SSEPs)N20 波振幅>4µV 或 EEG 内无放电的连续背景在 ROSC 后 72 小时内,以及 MRI 上皮质或深部灰质无弥散受限,在大多数研究中具有超过 80%的特异性和超过 40%的敏感性,预测良好的神经结局。大多数研究存在中度或高度偏倚风险。
在昏迷的心脏骤停幸存者中,临床、生物标志物、电生理学和影像学研究在心脏骤停后第一周内以高特异性识别出注定具有良好神经结局的患者。