Erdivanli Basar, Sen Ahmet, Batcik Sule, Koyuncu Tolga, Kazdal Hizir
Recep Tayyip Erdogan University, School of Medicine, Department of Anesthesiology and Reanimation, Rize, Turquia.
Recep Tayyip Erdogan University, School of Medicine, Department of Anesthesiology and Reanimation, Rize, Turquia.
Braz J Anesthesiol. 2018 Sep-Oct;68(5):499-506. doi: 10.1016/j.bjan.2018.04.003. Epub 2018 Jul 10.
We compared the efficiency of the King Vision video laryngoscope and the Macintosh laryngoscope, when used by experienced anesthesiologists on adult patients with varying intubating conditions, in a prospective randomized controlled clinical trial.
A total of 388 patients with an American Society of Anesthesiologists physical status of I or II, scheduled for general anesthesia with endotracheal intubation. Each patient was intubated with both laryngoscopes successively, in a randomized order. Intubation success rate, time to best glottic view, time to intubation, time to ventilation, Cormack–Lehane laryngoscopy grades, and complications related to the laryngoscopy and intubation were analyzed.
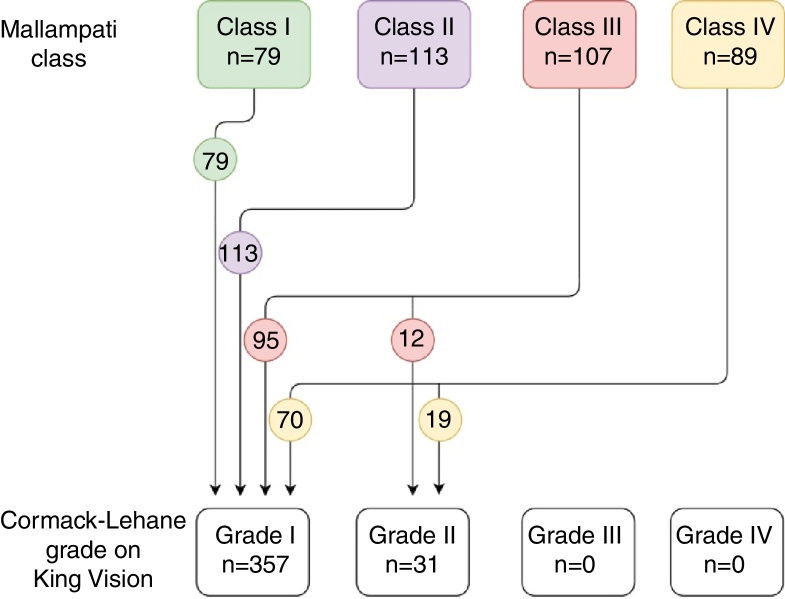
First pass intubation success rates were similar for the King Vision and the Macintosh (96.6% vs. 94.3%, respectively, > 0.05). King Vision resulted in a longer average time to glottic view (95% CI 0.5–1.4 s, < 0.001), and time to intubation (95% CI 3–4.6 s, < 0.001). The difference in time to intubation was similar when unsuccessful intubation attempts were excluded (95% CI 2.8–4.4 s, < 0.001). Based on the modified Mallampati class at the preoperative visit, the King Vision improved the glottic view in significantly more patients (220 patients, 56.7%) compared with the Macintosh (180 patients, 46.4%) ( < 0.001). None of the patients had peripheral oxygen desaturation below 94%. Experienced anesthesiologists may obtain similar rates of first pass intubation success and airway trauma with both laryngoscopes. King Vision requires longer times to visualize the glottis and to intubate the trachea, but does not cause additional desaturation.
在一项前瞻性随机对照临床试验中,我们比较了经验丰富的麻醉医生在不同插管条件的成年患者中使用可视喉镜(King Vision)和麦氏喉镜时的效率。
共有388例美国麻醉医师协会身体状况分级为Ⅰ或Ⅱ级、计划行气管插管全身麻醉的患者。每位患者先后使用两种喉镜进行插管,顺序随机。分析插管成功率、获得最佳声门视野的时间、插管时间、通气时间、Cormack-Lehane喉镜分级以及与喉镜检查和插管相关的并发症。
可视喉镜和麦氏喉镜的首次插管成功率相似(分别为96.6%和94.3%,P>0.05)。可视喉镜导致获得声门视野的平均时间更长(95%CI 0.5 - 1.4秒,P<0.001),插管时间更长(95%CI 3 - 4.6秒,P<0.001)。排除插管失败尝试后,插管时间差异相似(95%CI 2.8 - 4.4秒,P<0.001)。根据术前访视时改良的Mallampati分级,与麦氏喉镜(180例患者,46.4%)相比,可视喉镜使更多患者的声门视野得到改善(220例患者,56.7%)(P<0.001)。所有患者外周血氧饱和度均未低于94%。经验丰富的麻醉医生使用两种喉镜获得的首次插管成功率和气道损伤发生率相似。可视喉镜需要更长时间来观察声门和进行气管插管,但不会导致额外的血氧饱和度下降。