Gil-Barrionuevo Esther, Balibrea José Maria, Caubet Enric, Gonzalez Oscar, Vilallonga Ramón, Fort José Manuel, Ciudin Andrea, Armengol Manel
General Surgery Department, Vall d'Hebron University Hospital, Barcelona, Spain; Universitat Autònoma de Barcelona (UAB), Barcelona, Spain.
Endocrine, Metabolic and Bariatric Unit, General Surgery Department, Vall d'Hebron University Hospital, Barcelona, Spain; General Surgery Department, Vall d'Hebron University Hospital, Barcelona, Spain; Universitat Autònoma de Barcelona (UAB), Barcelona, Spain.
Int J Surg Case Rep. 2018;49:145-148. doi: 10.1016/j.ijscr.2018.06.024. Epub 2018 Jun 27.
Pheochromocytomas are infrequent tumors arised from the chromaphine cells of the adrenal sympathetic system. The excess of circulating catecholamines may lead to different cardiovascular disorders from silent alterations of the myocardial conduction to different forms of cardiomyopathy. The onset as cardiogenic shock is exceptional.
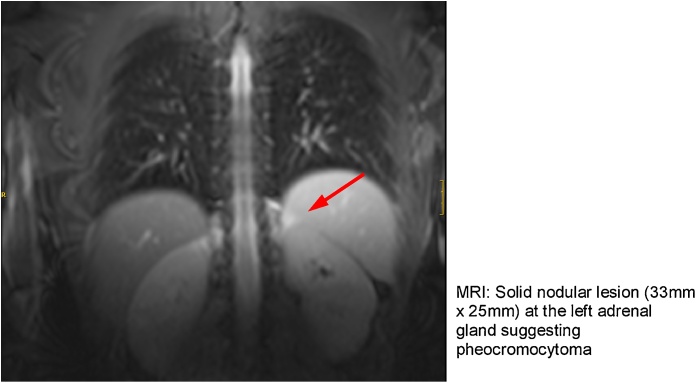
A 35-year-old male, with a known history of acute myopericarditis of unknown origin which debuted as acute pulmonary edema, was admitted with dyspnea in the context of a new heart failure episode with pulmonary edema. An initial ECG showed segmentary repolarization changes, reversed in subsequent ECGs. The echocardiogram showed severe left ventricular dysfunction and lateral and apical hypokinesia. Subsequent echocardiograms showed partial recovery of alterations and preserved systolic function. A cardiac MRI showed a subepicardial minimum catchment focus and myocardial edema suggestive of adrenergic myocarditis. A solid nodular lesion was found in the left adrenal gland, suggesting a pheochromocytoma. Laparoscopic left adrenalectomy confirmed a 30 mm adrenal tumor without signs of locoregional invasion. The patient had normal catecholamine excretion and heart function a few weeks after surgery. Histopathology confirmed the diagnosis of pheochromocytoma.
Adrenergic cardiomyopathy is a rare entity with a variable clinical presentation. The onset as cardiogenic shock is exceptional. The differential diagnosis of a patient with cardiogenic shock of unknown origin should consider the presence of an underlying pheocromocytoma as well as other states of adrenergic hyperstimulation. The reversibility of the myocardial affection in pheocromocytoma-associated myocardiopathy is common after the tumor resection.
嗜铬细胞瘤是起源于肾上腺交感神经系统嗜铬细胞的罕见肿瘤。循环中儿茶酚胺过量可能导致不同的心血管疾病,从心肌传导的隐匿改变到不同形式的心肌病。以心源性休克起病极为罕见。
一名35岁男性,有不明原因的急性心肌心包炎病史,最初表现为急性肺水肿,此次因新发心力衰竭伴肺水肿出现呼吸困难入院。初始心电图显示节段性复极改变,后续心电图恢复正常。超声心动图显示严重左心室功能障碍及侧壁和心尖运动减弱。后续超声心动图显示改变部分恢复且收缩功能保留。心脏磁共振成像显示心外膜下最小强化灶及提示肾上腺素能心肌炎的心肌水肿。左肾上腺发现实性结节性病变,提示嗜铬细胞瘤。腹腔镜下左肾上腺切除术证实为一个30毫米的肾上腺肿瘤,无局部侵犯迹象。术后几周患者儿茶酚胺排泄及心功能正常。组织病理学确诊为嗜铬细胞瘤。
肾上腺素能心肌病是一种临床表现多样的罕见疾病。以心源性休克起病极为罕见。不明原因的心源性休克患者的鉴别诊断应考虑潜在嗜铬细胞瘤的存在以及其他肾上腺素能过度刺激状态。嗜铬细胞瘤相关心肌病中心肌病变在肿瘤切除后通常可逆转。