Rehr Manuela, Shoaib Muhammad, Ellithy Sara, Okour Suhib, Ariti Cono, Ait-Bouziad Idriss, van den Bosch Paul, Deprade Anais, Altarawneh Mohammad, Shafei Abdel, Gabashneh Sadeq, Lenglet Annick
Médecins Sans Frontières, Operational Centre Amsterdam, Amman, Jordan.
2School of Medicine, Cardiff University, Cardiff, UK.
Confl Health. 2018 Jul 11;12:33. doi: 10.1186/s13031-018-0168-7. eCollection 2018.
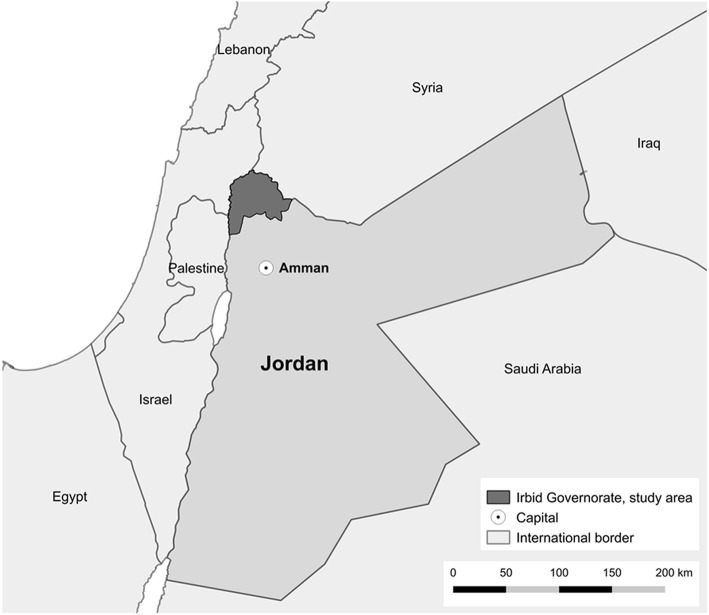
Tackling the high non-communicable disease (NCD) burden among Syrian refugees poses a challenge to humanitarian actors and host countries. Current response priorities are the identification and integration of key interventions for NCD care into humanitarian programs as well as sustainable financing. To provide evidence for effective NCD intervention planning, we conducted a cross-sectional survey among non-camp Syrian refugees in northern Jordan to investigate the burden and determinants for high NCDs prevalence and NCD multi-morbidities and assess the access to NCD care.
We used a two-stage cluster design with 329 randomly selected clusters and eight households identified through snowball sampling. Consenting households were interviewed about self-reported NCDs, NCD service utilization, and barriers to care.We estimated the adult prevalence of hypertension, diabetes type I/II, cardiovascular- and chronic respiratory conditions, thyroid disease and cancer and analysed the pattern of NCD multi-morbidities. We used the Cox proportional hazard model to calculate the prevalence ratios (PR) to analyse determinants for NCD prevalence and logistic regression to determine risk factors for NCD multi-morbidities by calculating odds ratios (ORs).
Among 8041 adults, 21.8%, (95% CI: 20.9-22.8) suffered from at least one NCD; hypertension (14.0, 95% CI: 13.2-14.8) and diabetes (9.2, 95% CI: 8.5-9.9) were the most prevalent NCDs. NCD multi-morbidities were reported by 44.7% (95% CI: 42.4-47.0) of patients. Higher age was associated with higher NCD prevalence and the risk for NCD-multi-morbidities; education was inversely associated.Of those patients who needed NCD care, 23.0% (95% CI: 20.5-25.6) did not seek it; 61.5% (95% CI: 54.7-67.9) cited provider cost as the main barrier. An NCD medication interruption was reported by 23.1% (95% CI: 20-4-26.1) of patients with regular medication needs; predominant reason was unaffordability (63.4, 95% CI: 56.7-69.6).
The burden of NCDs and multi-morbidities is high among Syrian refugees in northern Jordan. Elderly and those with a lower education are key target groups for NCD prevention and care, which informs NCD service planning and developing patient-centred approaches.Important unmet needs for NCD care exist; removing the main barriers to care could include cost-reduction for medications through humanitarian pricing models. Nevertheless, it is still essential that international donors agencies and countries fulfill their commitment to support the Syrian-crisis response.
应对叙利亚难民中高负担的非传染性疾病(NCD)对人道主义行为体和东道国构成了挑战。当前的应对重点是确定将非传染性疾病护理的关键干预措施纳入人道主义项目并实现可持续融资。为了为有效的非传染性疾病干预规划提供证据,我们在约旦北部的非营地叙利亚难民中进行了一项横断面调查,以调查非传染性疾病高患病率和非传染性疾病多重共病的负担及决定因素,并评估获得非传染性疾病护理的情况。
我们采用两阶段整群设计,随机选择329个群组,并通过雪球抽样确定8个家庭。对同意参与的家庭就自我报告的非传染性疾病、非传染性疾病服务利用情况和护理障碍进行访谈。我们估计了高血压、I/II型糖尿病、心血管和慢性呼吸道疾病、甲状腺疾病和癌症的成人患病率,并分析了非传染性疾病多重共病的模式。我们使用Cox比例风险模型计算患病率比(PR),以分析非传染性疾病患病率的决定因素,并使用逻辑回归通过计算比值比(OR)来确定非传染性疾病多重共病的风险因素。
在8041名成年人中,21.8%(95%置信区间:20.9 - 22.8)患有至少一种非传染性疾病;高血压(14.0,95%置信区间:13.2 - 14.8)和糖尿病(9.2,95%置信区间:8.5 - 9.9)是最常见的非传染性疾病。44.7%(95%置信区间:42.4 - 47.0)的患者报告有非传染性疾病多重共病。年龄越大,非传染性疾病患病率和非传染性疾病多重共病风险越高;教育程度与之呈负相关。在需要非传染性疾病护理的患者中,23.0%(95%置信区间:20.5 - 25.6)未寻求护理;61.5%(95%置信区间:54.7 - 67.9)表示提供者费用是主要障碍。23.1%(95%置信区间:20.4 - 26.1)有定期用药需求的患者报告有非传染性疾病药物中断情况;主要原因是负担不起(63.4,95%置信区间:56.7 - 69.6)。
约旦北部叙利亚难民中非传染性疾病和多重共病的负担很高。老年人和教育程度较低者是非传染性疾病预防和护理的关键目标群体,这为非传染性疾病服务规划和制定以患者为中心的方法提供了依据。非传染性疾病护理存在重要的未满足需求;消除主要护理障碍可包括通过人道主义定价模式降低药物成本。尽管如此,国际捐助机构和国家履行其支持叙利亚危机应对的承诺仍然至关重要。