Chen Yahua, Chen Yangyang, Chen Xiaoqiong, Chen Liang, Liang Wei
Department of Gastroenterology, Affiliated Hospital of Putian University, and Affiliated Putian Hospital of Southern Medical University, Putian, Fujian 351100, P.R. China.
Department of Gastrointestinal Endoscopy, Fujian Provincial Hospital, Teaching Hospital of Fujian Medical University, Fuzhou, Fujian 350001, P.R. China.
Oncol Lett. 2018 Aug;16(2):1419-1424. doi: 10.3892/ol.2018.8811. Epub 2018 May 25.
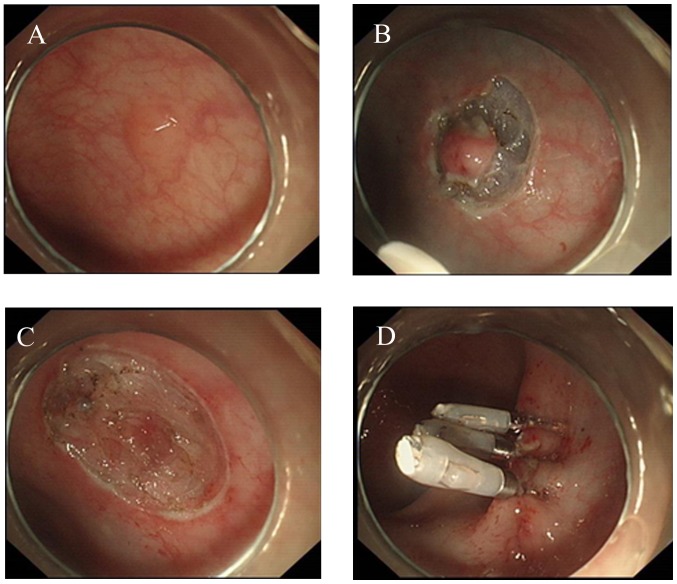
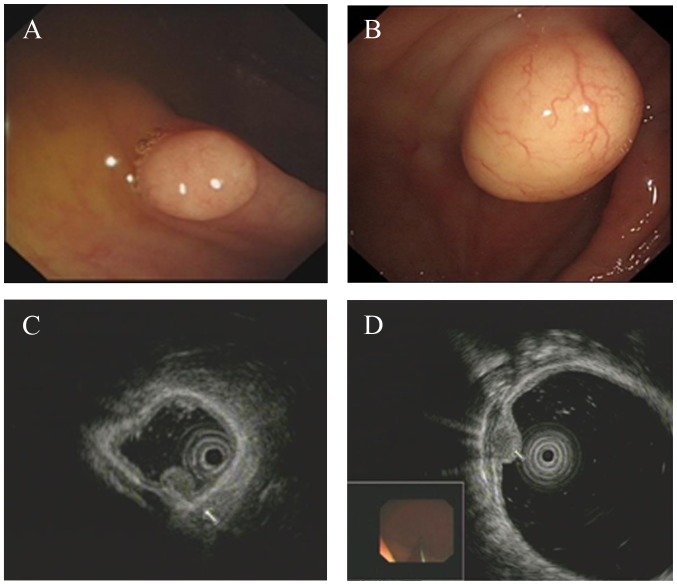
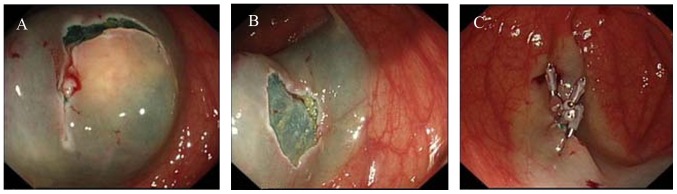
Colonic granular cell tumors (GCTs) are rare and benign, but have malignant potential. The recent progress in endoscopic procedures and technology facilitate the diagnosis and treatment of GCTs. The present study described 11 cases of colonic GCTs diagnosed between March 2010 and April 2015, including patient clinical and histopathological features. Patients were generally asymptomatic. The most common symptoms were hematoquezia and abdominal pain. The male/female ratio was 7:4; age range was 40-67 years. Colonoscopy revealed a yellowish or white, solid and well-circumscribed tumor covered by normal mucosa. Endoscopic ultrasonography (EUS) showed a homogenous, or granular-type heterogeneous, hypoechoic solid tumor originating from the submucosal layer (8 cases) or muscularis mucosae (3 cases), with maximum diameters 0.3-3.0 cm. All patients underwent endoscopic submucosal dissection or endoscopic submucosal excavation without complication. All tumors were block removed. The mean operative time was 38 min (range, 31-50 min). Immunohistochemical analysis of all specimens confirmed the diagnosis of GCT by positive staining of S-100 protein. No recurrence or metastasis was observed during follow-up periods of 11 months to 5 years. In conclusion, colonoscopy, EUS and immunohistological examination increase the accuracy of diagnosis of GCTs. Endoscopic management is feasible and safe for GCT treatment.
结肠颗粒细胞瘤(GCTs)罕见且为良性,但有恶变潜能。内镜诊疗程序和技术的最新进展促进了GCTs的诊断与治疗。本研究描述了2010年3月至2015年4月期间诊断的11例结肠GCTs,包括患者的临床和组织病理学特征。患者通常无症状。最常见的症状是便血和腹痛。男女比例为7:4;年龄范围为40 - 67岁。结肠镜检查显示一个淡黄色或白色、实性且边界清晰的肿瘤,表面覆盖正常黏膜。内镜超声检查(EUS)显示一个均匀的或颗粒型不均匀的低回声实性肿瘤,起源于黏膜下层(8例)或黏膜肌层(3例),最大直径为0.3 - 3.0 cm。所有患者均接受了内镜黏膜下剥离术或内镜黏膜下挖除术,无并发症发生。所有肿瘤均整块切除。平均手术时间为38分钟(范围为31 - 50分钟)。所有标本的免疫组织化学分析通过S - 100蛋白阳性染色确诊为GCT。在11个月至5年的随访期间未观察到复发或转移。总之,结肠镜检查、EUS和免疫组织学检查提高了GCTs的诊断准确性。内镜治疗对GCTs的治疗是可行且安全的。