Sakata Kenneth K, Azadeh Natalya, Brighton Anjuli, Temkit M'hamed, Klassen Christine L, Grys Thomas E, Vikram Holenarasipur R
Division of Pulmonary Medicine, Mayo Clinic, Phoenix, AZ, USA.
Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN, USA.
Can Respir J. 2018 Jun 13;2018:9821426. doi: 10.1155/2018/9821426. eCollection 2018.
To determine whether results of the nasopharyngeal FilmArray respiratory panel (NP-FARP) influenced antibiotic decisions.
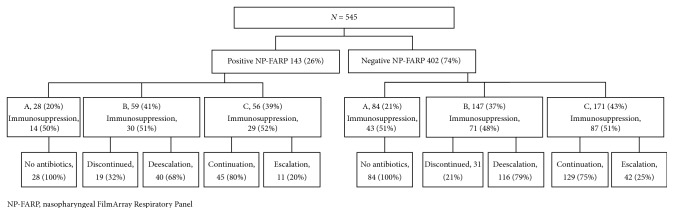
We reviewed the medical records of nonintensive care unit (ICU) inpatients that had an NP-FARP performed at our institution between June 2013 and June 2014. The inpatient records were reviewed 48 hours after the NP-FARP for the following data: demographic information; NP-FARP, serum procalcitonin, and methicillin-resistant nasal swab (MRSA NS) results; antibiotics prior and post-48 hours of the NP-FARP result; and the current immunosuppression status. Clinical outcome data were not obtained. Patients were categorized into those who had a positive (+) or a negative (-) NP-FARP. We further subdivided these two categories into groups A, B, and C based on the antibiotic modifications 48 hours after their NP-FARP result. Group A included patients who were never initiated on antimicrobial therapy. Patients whose antibiotics were discontinued or deescalated were placed in group B. Patients with antibiotic escalation or continuation without change constituted group C. We compared and analyzed groups A, B, and C in the (+) and (-) NP-FARP cohorts.
A total of 545 patients were included. There were 143 (26%) patients with positive and 402 (74%) patients with negative NP-FARPs. Comparison of groups A, B, and C between those with a (+) and (-) NP-FARP were as follows: (+) A and (-) A, 28/143 (20%) and 84/402 (21%); (+) B and (-) B, 59/143 (41%) and 147/402 (37%); and (+) C and (-) C, 56/143 (39%) and 171/402 (43%), respectively. We found no statistically significant differences between groups (+) A versus (-) A, (+) B versus (-) B, and (+) C versus (-) C with respect to age, gender, MRSA NS result, procalcitonin result, or concurrent immunosuppression.
In non-ICU inpatients, NP-FARP alone or in combination with procalcitonin or MRSA NS did not influence antibiotic decisions during the study period.
确定鼻咽部FilmArray呼吸道病原体检测板(NP-FARP)的检测结果是否会影响抗生素的使用决策。
我们回顾了2013年6月至2014年6月期间在我院接受NP-FARP检测的非重症监护病房(ICU)住院患者的病历。在NP-FARP检测48小时后,对住院病历进行如下数据审查:人口统计学信息;NP-FARP、血清降钙素原和耐甲氧西林鼻拭子(MRSA NS)检测结果;NP-FARP检测结果出现前后48小时内使用的抗生素;以及当前的免疫抑制状态。未获取临床结局数据。将患者分为NP-FARP检测结果为阳性(+)或阴性(-)的两组。根据NP-FARP检测结果48小时后的抗生素调整情况,我们将这两组进一步细分为A、B、C三组。A组包括从未接受过抗菌治疗的患者。抗生素停用或降级的患者归入B组。抗生素升级或持续使用且未改变的患者构成C组。我们对NP-FARP检测结果为阳性(+)和阴性(-)的队列中的A、B、C三组进行了比较和分析。
共纳入545例患者。其中NP-FARP检测结果为阳性的患者有143例(26%),检测结果为阴性的患者有402例(74%)。NP-FARP检测结果为阳性(+)和阴性(-)的患者中,A、B、C三组的比较情况如下:(+)A组与(-)A组,分别为28/143(20%)和84/402(21%);(+)B组与(-)B组,分别为59/143(41%)和147/402(37%);(+)C组与(-)C组,分别为56/143(39%)和171/402(43%)。我们发现,在年龄、性别、MRSA NS检测结果、降钙素原检测结果或同时存在的免疫抑制方面,(+)A组与(-)A组、(+)B组与(-)B组、(+)C组与(-)C组之间均无统计学显著差异。
在非ICU住院患者中,在研究期间,单独使用NP-FARP或联合降钙素原或MRSA NS检测均未影响抗生素的使用决策。