KEMRI-Wellcome Trust Research Programme, Nairobi, Kenya.
University of Nairobi, Department of Paediatrics and Child Health, Nairobi, Kenya.
BMC Infect Dis. 2018 Jul 16;18(1):328. doi: 10.1186/s12879-018-3237-z.
Globally, 40% of all tuberculosis (TB) cases, 65% paediatric cases and 75% multi-drug resistant TB (MDR-TB) cases are missed due to underreporting and/or under diagnosis. A recent Kenyan TB prevalence survey found that a significant number of TB cases are being missed here. Understanding spatial distribution and patterns of use of TB diagnostic tests as per the guidelines could potentially help improve TB case detection by identifying diagnostic gaps.
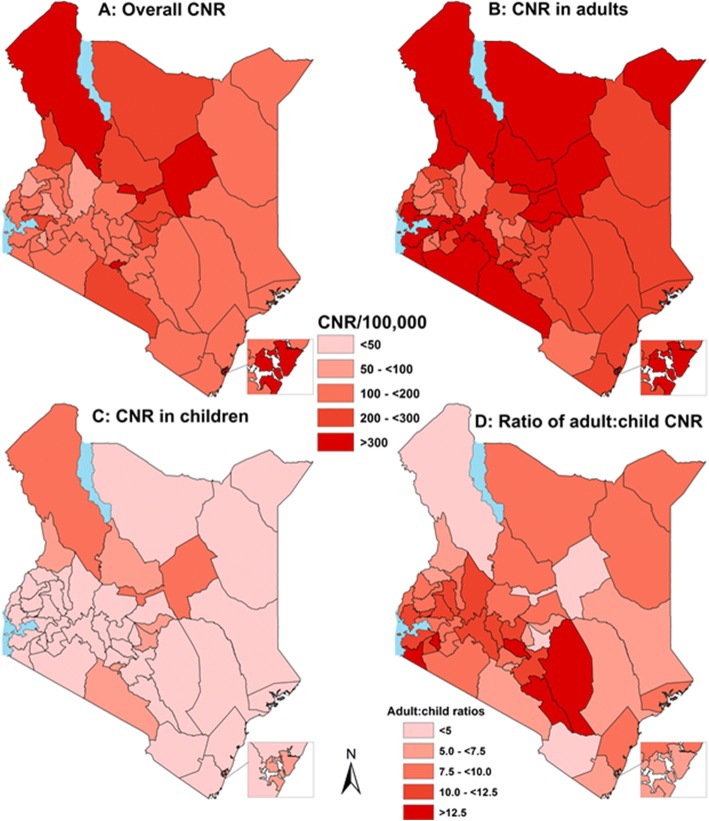
We used 2015 Kenya National TB programme data to map TB case notification rates (CNR) in different counties, linked with their capacity to perform diagnostic tests (chest x-rays, smear microscopy, Xpert MTB/RIF®, culture and line probe assay). We then ran hierarchical regression models for adults and children to specifically establish determinants of use of Xpert® (as per Kenyan guidelines) with county and facility as random effects.
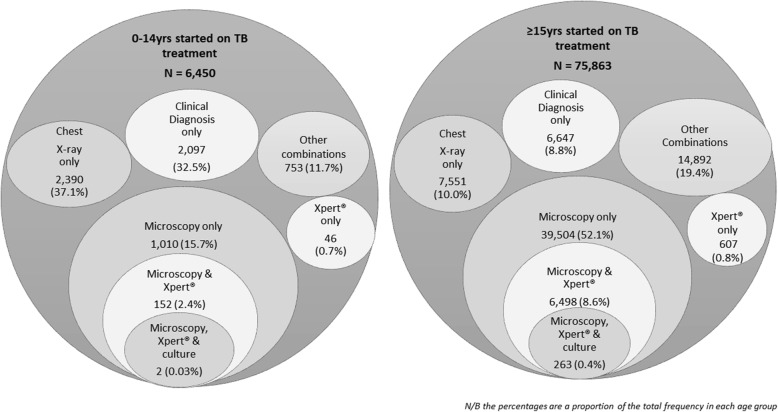
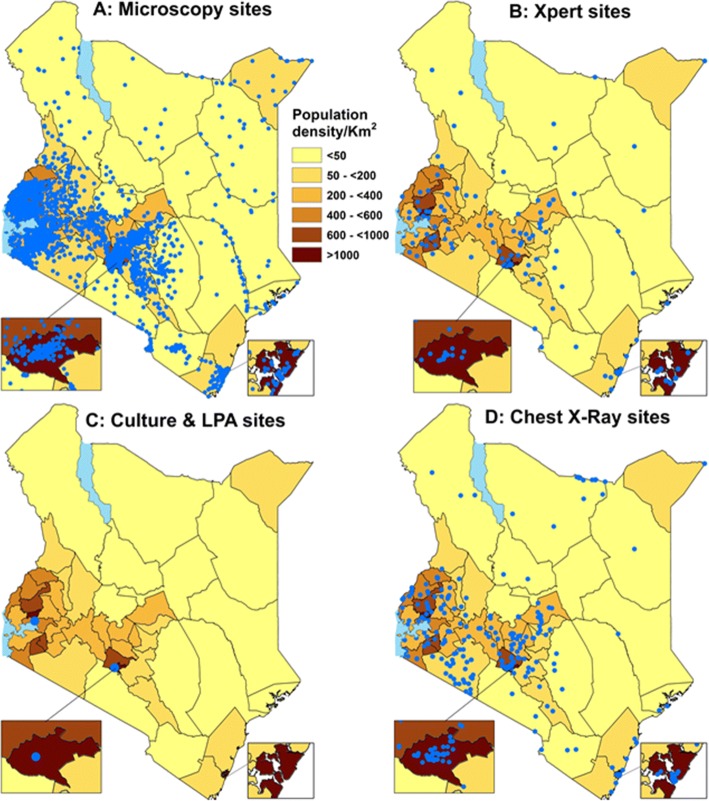
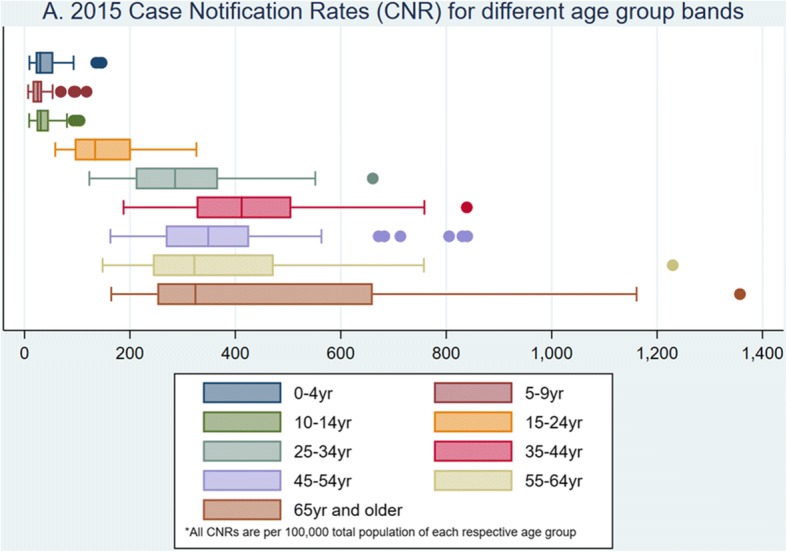
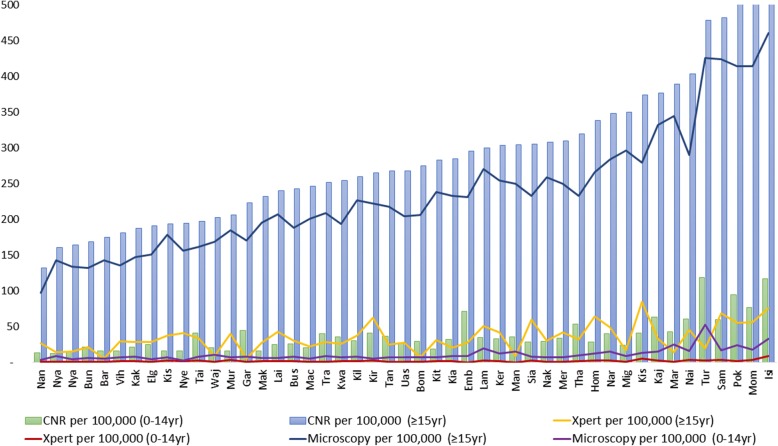
In 2015, 82,313 TB cases were notified and 7.8% were children. The median CNR/100,000 amongst 0-14yr olds was 37.2 (IQR 20.6, 41.0) and 267.4 (IQR 202.6, 338.1) for ≥15yr olds respectively. 4.8% of child TB cases and 12.2% of adult TB cases had an Xpert® test done, with gaps in guideline adherence. There were 2,072 microscopy sites (mean microscopy density 4.46/100,000); 129 Xpert® sites (mean 0.31/100,000); two TB culture laboratories and 304 chest X-ray facilities (mean 0.74/100,000) with variability in spatial distribution across the 47 counties. Retreatment cases (i.e. failures, relapses/recurrences, defaulters) had the highest odds of getting an Xpert® test compared to new/transfer-in patients (AOR 7.81, 95% CI 7.33-8.33). Children had reduced odds of getting an Xpert® (AOR 0.41, CI 0.36-0.47). HIV-positive individuals had nearly twice the odds of getting an Xpert® test (AOR 1.82, CI 1.73-1.92). Private sector and higher-level hospitals had a tendency towards lower odds of use of Xpert®.
We noted under-use and gaps in guideline adherence for Xpert® especially in children. The under-use despite considerable investment undermines cost-effectiveness of Xpert®. Further research is needed to develop strategies enhancing use of diagnostics, including innovations to improve access (e.g. specimen referral) and overcoming local barriers to adoption of guidelines and technologies.
在全球范围内,40%的结核病(TB)病例、65%的儿科病例和 75%的耐多药结核病(MDR-TB)病例由于漏报和/或漏诊而未被发现。最近肯尼亚的一项结核病患病率调查发现,这里有相当数量的结核病病例未被发现。了解按照指南使用结核病诊断检测的空间分布和模式,可能有助于通过确定诊断差距来提高结核病病例的检出率。
我们使用了 2015 年肯尼亚国家结核病规划数据,根据其开展诊断检测的能力(胸部 X 光、涂片显微镜检查、Xpert MTB/RIF®、培养和线探针检测),在不同县对结核病病例通报率(CNR)进行了绘图。然后,我们针对成人和儿童运行了分层回归模型,特别是根据肯尼亚的指南,以县和医疗机构为随机效应,确定使用 Xpert®的决定因素。
2015 年,共通报了 82313 例结核病病例,其中 7.8%为儿童。0-14 岁儿童的中位 CNR/100000 分别为 37.2(20.6-41.0)和 267.4(202.6-338.1)。4.8%的儿童结核病病例和 12.2%的成人结核病病例接受了 Xpert®检测,而且未完全遵循指南。有 2072 个显微镜检测点(平均显微镜检测密度为每 100000 人 4.46 个);129 个 Xpert®检测点(平均每 100000 人 0.31 个);2 个结核培养实验室和 304 个胸部 X 光设备(平均每 100000 人 0.74 个),47 个县的空间分布存在差异。复治病例(即失败、复发/再发、失访)与新病例/转入病例相比,接受 Xpert®检测的可能性最高(优势比 7.81,95%置信区间 7.33-8.33)。儿童接受 Xpert®检测的可能性降低(优势比 0.41,95%置信区间 0.36-0.47)。HIV 阳性个体接受 Xpert®检测的可能性几乎增加了一倍(优势比 1.82,95%置信区间 1.73-1.92)。私营部门和高级别医院使用 Xpert®的可能性较低。
我们注意到,特别是在儿童中,Xpert®的使用不足且未完全遵循指南。尽管投入了大量资金,但 Xpert®的使用不足破坏了其成本效益。需要进一步研究,以制定增强诊断检测使用的策略,包括创新措施来改善获取途径(例如标本转介),并克服采用指南和技术的地方障碍。