Department of Vascular and Endovascular Surgery, Royal Free Hospital, London, UK.
Department of Vascular Surgery, New York University Langone Medical Center, New York, USA.
Stroke Vasc Neurol. 2018 Feb 24;3(2):92-100. doi: 10.1136/svn-2017-000129. eCollection 2018 Jun.
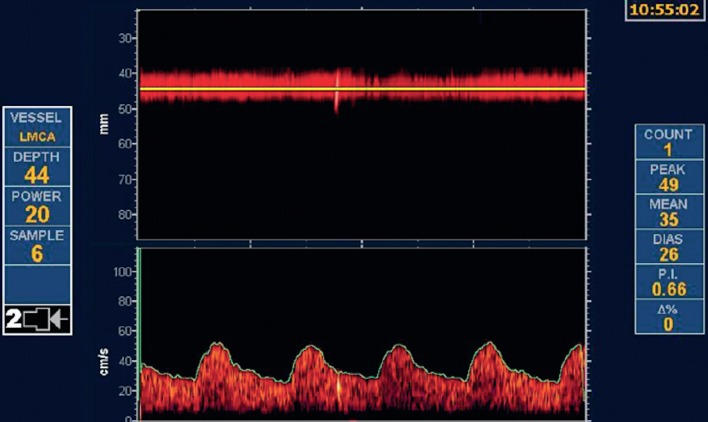
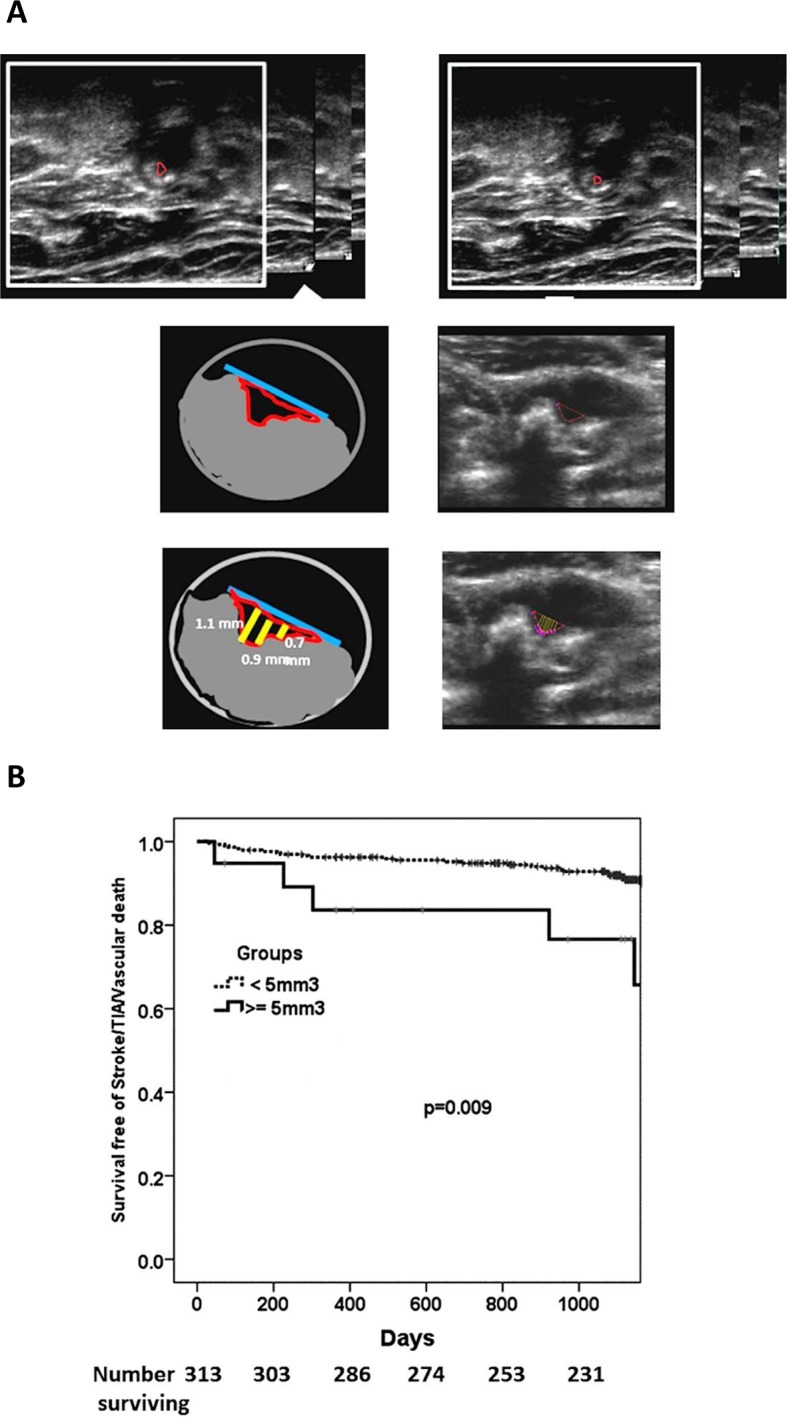
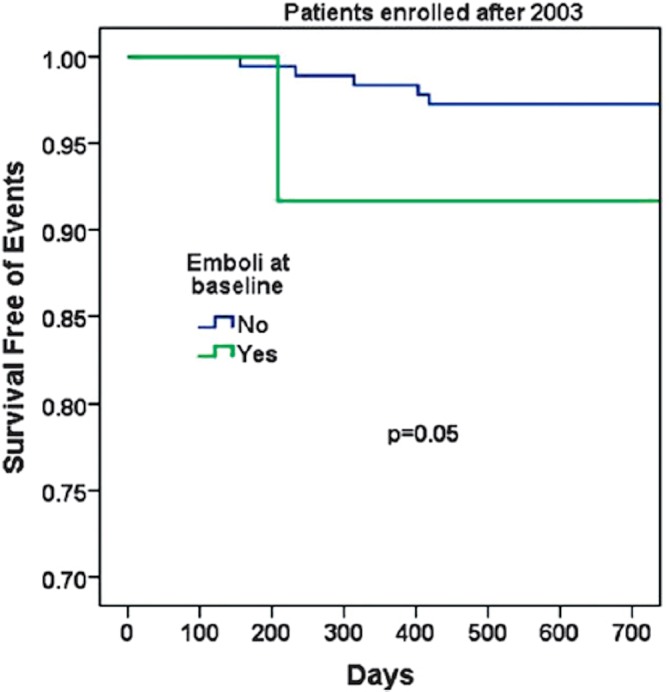
Offering routine carotid endarterectomy (CEA) or carotid artery stenting (CAS) to patients with asymptomatic carotid artery stenosis (ACS) is no longer considered as the optimal management of these patients. Equally suboptimal, however, is the policy of offering only best medical treatment (BMT) to all patients with ACS and not considering any of them for prophylactic CEA. In the last few years, there have been many studies aiming to identify reliable predictors of future cerebrovascular events that would allow the identification of patients with high-risk ACS and offer a prophylactic carotid intervention only to these patients to prevent them from becoming symptomatic. All patients with ACS should receive BMT. The present article will summarise the evidence suggesting ways to identify these high-risk asymptomatic individuals, namely: (1) microemboli detection on transcranial Doppler, (2) plaque echolucency on Duplex ultrasound, (3) progression in the severity of ACS, (4) silent embolic infarcts on brain CT/MRI, (5) reduced cerebrovascular reserve, (6) increased size of juxtaluminal hypoechoic area, (7) identification of intraplaque haemorrhage using MRI and (8) carotid ulceration. The evidence suggests that approximately 10%-15% of patents with asymptomatic stenosis might benefit from intervention; this will become more clear after publication of ongoing studies comparing stenting or endarterectomy with best medical therapy. In the meantime, no patient should be offered intervention unless there is evidence of high risk of ipsilateral stroke, from modalities such as those discussed here.
对于无症状颈动脉狭窄(ACS)患者,不再常规行颈动脉内膜切除术(CEA)或颈动脉支架置入术(CAS),目前认为这并非此类患者的最佳治疗方案。同样不理想的是,对于所有 ACS 患者,仅给予最佳药物治疗(BMT),而不考虑对其进行预防性 CEA 的策略。近年来,已有许多研究旨在确定可靠的未来脑血管事件预测因子,以识别高危 ACS 患者,并仅对这些患者进行预防性颈动脉介入治疗,以防止其出现症状。所有 ACS 患者均应接受 BMT。本文将总结提示识别这些高危无症状个体的证据,包括:(1)经颅多普勒检测微栓子;(2)双功能超声检测斑块不匀质回声;(3)ACS 严重程度进展;(4)脑 CT/MRI 显示无症状栓塞性梗死;(5)脑血流储备减少;(6)管腔外低回声区增大;(7)使用 MRI 识别斑块内出血;(8)颈动脉溃疡。有证据表明,约 10%-15%的无症状狭窄患者可能从介入治疗中获益;这将在比较支架置入术或内膜切除术与最佳药物治疗的正在进行的研究发表后变得更加明确。在此期间,除非有同侧卒中的高危证据(如这里讨论的这些方法),否则不应向任何患者提供介入治疗。