Winters Z E, Horsnell J, Elvers K T, Maxwell A J, Jones L J, Shaaban A M, Schmid P, Williams N R, Beswick A, Greenwood R, Ingram J C, Saunders C, Vaidya J S, Esserman L, Jatoi I, Brunt A M
Patient-Reported and Clinical Outcomes Research Group Surgical and Interventional Trials Unit (SITU) London UK.
Department of Breast Surgery Royal Surrey County Hospital NHS Foundation Trust Guildford UK.
BJS Open. 2018 May 22;2(4):162-174. doi: 10.1002/bjs5.53. eCollection 2018 Aug.
The clinical effectiveness of treating ipsilateral multifocal (MF) and multicentric (MC) breast cancers using breast-conserving surgery (BCS) compared with the standard of mastectomy is uncertain. Inconsistencies relate to definitions, incidence, staging and intertumoral heterogeneity. The primary aim of this systematic review was to compare clinical outcomes after BCS versus mastectomy for MF and MC cancers, collectively defined as multiple ipsilateral breast cancers (MIBC).
Comprehensive electronic searches were undertaken to identify complete papers published in English between May 1988 and July 2015, primarily comparing clinical outcomes of BCS and mastectomy for MIBC. All study designs were included, and studies were appraised critically using the Newcastle-Ottawa Scale. The characteristics and results of identified studies were summarized.
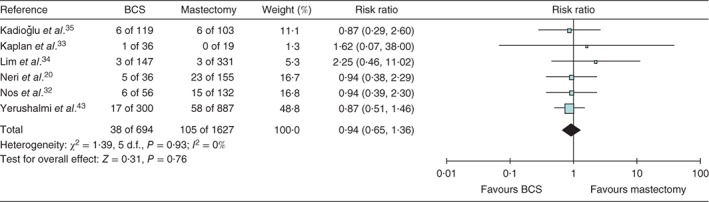
Twenty-four retrospective studies were included in the review: 17 comparative studies and seven case series. They included 3537 women with MIBC undergoing BCS; breast cancers were defined as MF in 2677 women, MC in 292, and reported as MIBC in 568. Six studies evaluated MIBC treated by BCS or mastectomy, with locoregional recurrence (LRR) rates of 2-23 per cent after BCS at median follow-up of 59·5 (i.q.r. 56-81) months. BCS and mastectomy showed apparently equivalent rates of LRR (risk ratio 0·94, 95 per cent c.i. 0·65 to 1·36). Thirteen studies compared BCS in women with MIBC versus those with unifocal cancers, reporting LRR rates of 2-40 per cent after BCS at a median follow-up of 64 (i.q.r. 57-73) months. One high-quality study reported 10-year actuarial LRR rates of 5·5 per cent for BCS in 300 women versus 6·5 per cent for mastectomy among 887 women.
The available studies were mainly of moderate quality, historical and underpowered, with limited follow-up and biased case selection favouring BCS rather than mastectomy for low-risk patients. The evidence was inconclusive, weakening support for the St Gallen consensus and supporting a future randomized trial.
与标准乳房切除术相比,采用保乳手术(BCS)治疗同侧多灶性(MF)和多中心性(MC)乳腺癌的临床疗效尚不确定。不一致之处涉及定义、发病率、分期和肿瘤间异质性。本系统评价的主要目的是比较BCS与乳房切除术治疗MF和MC癌症(统称为同侧多原发性乳腺癌(MIBC))后的临床结局。
进行全面的电子检索,以识别1988年5月至2015年7月期间以英文发表的完整论文,主要比较BCS和乳房切除术治疗MIBC的临床结局。纳入所有研究设计,并使用纽卡斯尔-渥太华量表对研究进行严格评估。总结已识别研究的特征和结果。
本评价纳入了24项回顾性研究:17项比较研究和7个病例系列。其中包括3537例接受BCS的MIBC女性患者;2677例女性患者的乳腺癌被定义为MF,292例为MC,568例报告为MIBC。6项研究评估了接受BCS或乳房切除术治疗的MIBC,BCS组中位随访59.5(四分位间距56 - 81)个月后的局部区域复发(LRR)率为2% - 23%。BCS和乳房切除术的LRR率似乎相当(风险比0.94,95%置信区间0.65至1.36)。13项研究比较了MIBC女性与单灶性癌症女性接受BCS的情况,BCS组中位随访64(四分位间距57 - 73)个月后的LRR率为2% - 40%。一项高质量研究报告,300例接受BCS的女性10年精算LRR率为5.5%,而887例接受乳房切除术的女性为6.5%。
现有研究质量主要为中等,多为历史性研究且效能不足,随访有限,病例选择存在偏倚,倾向于对低风险患者采用BCS而非乳房切除术。证据尚无定论,削弱了对圣加仑共识的支持,并支持未来进行随机试验。