Drury Nigel E, Horsburgh Angela, Bi Rehana, Willetts Robert G, Jones Timothy J
1 Department of Paediatric Cardiac Surgery, Birmingham Children's Hospital, Birmingham, UK.
2 Institute of Cardiovascular Sciences, University of Birmingham, Birmingham, UK.
Perfusion. 2019 Mar;34(2):125-129. doi: 10.1177/0267659118794343. Epub 2018 Aug 10.
Many techniques are available for cardioplegic arrest in children, but there is a lack of late phase clinical trials to guide practice. We surveyed paediatric cardiac surgeons and perfusionists to establish current practice and willingness to change within a clinical trial.
An online survey was sent to all consultant paediatric cardiac surgeons and chief perfusionists in paediatric centres in the UK and Ireland. Information was sought on cardioplegia type, composition, temperature, topical cooling, dosing for induction and maintenance, interval between doses, whether practice changed with patient age or complexity and whether respondents would be willing and able to use different cardioplegia solutions within a randomised trial.
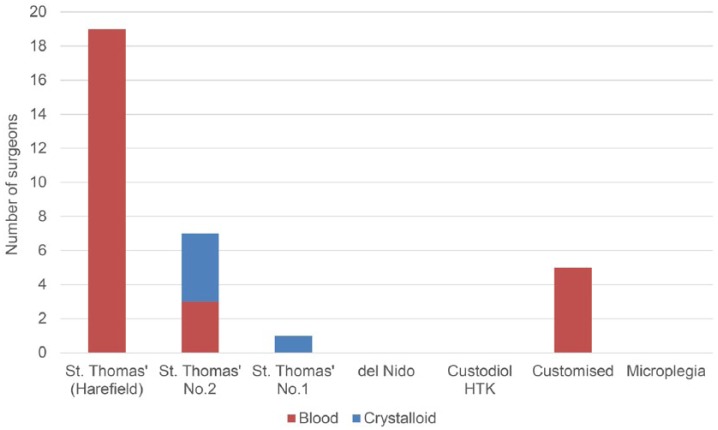
Responses were obtained from 32 (78.0%) surgeons and 12 (100%) perfusionists. Twenty-seven (84.4%) surgeons use blood cardioplegia in infants, with St. Thomas' Harefield preparation the most popular (19, 59.4%), used routinely in eight (66.7%) centres. Twenty-two (68.8%) administer at 4-6°C, 18 (56.3%) use topical cooling, 18 (56.3%) give 30 ml/kg induction and 15 ml/kg maintenance, with 23 (71.9%) re-dosing every 20-25 minutes. Thirty (93.8%) surgeons were open to randomising patients in a trial, with del Nido (29, 90.6%) the most popular.
This survey demonstrates heterogeneity in cardioplegia practice. Whilst most surgeons use blood cardioplegia, there is variation in type, temperature, topical cooling, dosing and intervals. Combined with a lack of evidence from late phase trials, our findings support the presence of clinical equipoise. Surgeons are willing to change practice, suggesting that a pragmatic, multi-centre, randomised, controlled trial of cardioplegia in children is feasible.
儿童心脏停搏有多种技术可用,但缺乏后期临床试验来指导实践。我们对儿科心脏外科医生和灌注师进行了调查,以确定当前的实践情况以及在临床试验中改变的意愿。
向英国和爱尔兰儿科中心的所有儿科心脏外科顾问医生和首席灌注师发送了在线调查问卷。收集了关于心脏停搏液类型、成分、温度、局部降温、诱导和维持剂量、给药间隔、实践是否随患者年龄或病情复杂程度而改变以及受访者是否愿意并能够在随机试验中使用不同心脏停搏液的信息。
32名(78.0%)外科医生和12名(100%)灌注师回复了问卷。27名(84.4%)外科医生在婴儿中使用血液心脏停搏液,其中圣托马斯医院 - 哈雷菲尔德配方最受欢迎(19名,59.4%),8个(66.7%)中心常规使用。22名(68.8%)在4 - 6°C给药,18名(56.3%)使用局部降温,18名(56.3%)给予30ml/kg诱导剂量和15ml/kg维持剂量,23名(71.9%)每20 - 25分钟重复给药一次。30名(93.8%)外科医生愿意在试验中对患者进行随机分组,德尔尼多配方(29名,90.6%)最受欢迎。
本次调查表明心脏停搏实践存在异质性。虽然大多数外科医生使用血液心脏停搏液,但在类型、温度、局部降温、剂量和间隔方面存在差异。结合后期试验缺乏证据,我们的研究结果支持存在临床平衡。外科医生愿意改变实践,这表明针对儿童心脏停搏进行务实的多中心随机对照试验是可行的。