Evans Marc, Mehta Roopa, Gundgaard Jens, Chubb Barrie
University Hospital Llandough, Penarth, Cardiff, UK.
Departamento de Endocrinologia y Metabolismo, Instituto Nacional de Ciencias Médicas y Nutricion Salvador Zubiran, Vasco de Quiroga 15, Mexico City, Mexico.
Diabetes Ther. 2018 Oct;9(5):1919-1930. doi: 10.1007/s13300-018-0478-1. Epub 2018 Aug 10.
Understanding which therapeutic innovations in diabetes represent the best value requires rigorous economic evaluation. Data from randomised controlled trials and observational studies indicate that insulin degludec has a hypoglycemia advantage versus insulin glargine 100 units/mL (glargine U100), the most widely prescribed basal insulin analogue in the UK. This analysis was done to more rigorously assess cost-effectiveness in a UK setting.
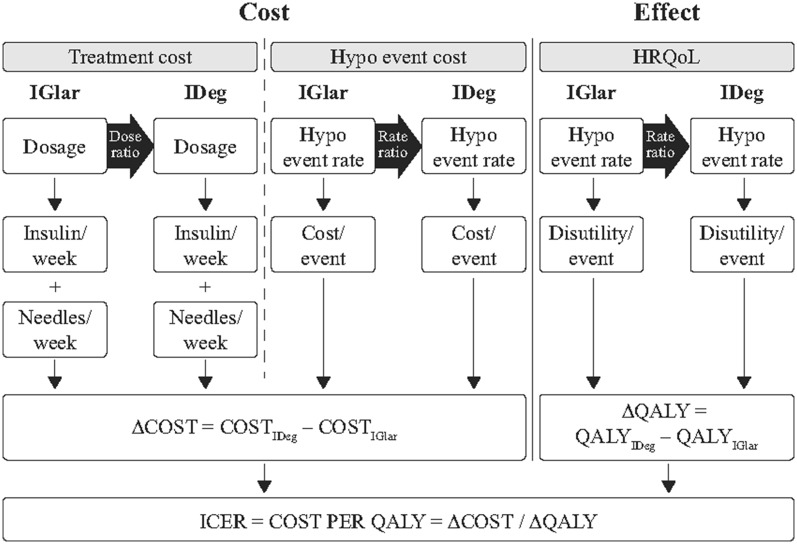
Data from two double-blinded, randomised, two-period crossover trials in type 1 (SWITCH 1) and type 2 (SWITCH 2) diabetes mellitus were used to assess the cost-effectiveness of degludec vs. glargine U100 with an economic model. Cost-effectiveness was analysed over a 1-year time horizon based on the different rates of hypoglycaemia and actual doses of insulin used, rather than glycaemic control due to the treat-to-target trial design.
In type 1 diabetes mellitus, degludec was highly cost-effective compared with glargine U100, with an incremental cost-effectiveness ratio of £984 (increased costs of only £23/year and improvement in participant health of 0.0232 quality-adjusted life-years (QALYs)). In type 2 diabetes mellitus, it was estimated that quality of life was improved (0.0065 QALYs gain) with degludec compared with glargine U100 at an increased annual cost of £117 (incremental cost-effectiveness ratio, £17,939). One-way sensitivity analyses showed that the results were robust to changes in parameters in both type 1 and type 2 diabetes mellitus.
The rigorous design of the SWITCH trials, coupled with a representative patient population and a definition of hypoglycaemia that is relevant for real-world patients, makes the results of these trials highly generalisable. The within-trial analysis has the added value of being able to include doses and event rates directly from the trials. This short-term economic analysis estimated that IDeg would be cost-effective relative to IGlar U100 in both type 1 and type 2 diabetes mellitus in the UK.
SWITCH 1 (NCT02034513); SWITCH 2 (NCT02030600).
Novo Nordisk, Søborg, Denmark.
了解糖尿病领域哪些治疗创新具有最佳价值需要进行严格的经济学评估。随机对照试验和观察性研究的数据表明,与甘精胰岛素100单位/毫升(甘精胰岛素U100,英国处方量最大的基础胰岛素类似物)相比,德谷胰岛素具有低血糖优势。开展此项分析是为了在英国背景下更严格地评估成本效益。
利用两项针对1型糖尿病(SWITCH 1)和2型糖尿病(SWITCH 2)的双盲、随机、两阶段交叉试验的数据,通过经济模型评估德谷胰岛素与甘精胰岛素U100的成本效益。基于低血糖发生率和实际使用的胰岛素剂量,而非因达标治疗试验设计所带来的血糖控制情况,在1年时间范围内分析成本效益。
在1型糖尿病中,与甘精胰岛素U100相比,德谷胰岛素具有很高的成本效益,增量成本效益比为984英镑(每年成本仅增加23英镑,患者健康改善0.0232个质量调整生命年(QALY))。在2型糖尿病中,估计与甘精胰岛素U100相比,德谷胰岛素可改善生活质量(获得0.0065个QALY),但每年成本增加117英镑(增量成本效益比为17,939英镑)。单向敏感性分析表明,1型和2型糖尿病中参数的变化对结果影响不大。
SWITCH试验的严格设计,加上具有代表性的患者群体以及与现实世界患者相关的低血糖定义,使得这些试验结果具有很高的普遍性。试验内分析的附加价值在于能够直接纳入试验中的剂量和事件发生率。这项短期经济学分析估计,在英国,1型和2型糖尿病中,相对于甘精胰岛素U100而言,德谷胰岛素具有成本效益。
SWITCH 1(NCT02034513);SWITCH 2(NCT02030600)。
丹麦诺和诺德公司,斯堡。