Gulati Swati, Zouk Aline N, Kalehoff Jonathan P, Wren Christopher S, Davison Peter N, Kirkpatrick Denay Porter, Bhatt Surya P, Dransfield Mark T, Wells James Michael
Department of Medicine, University of Alabama at Birmingham (UAB), Birmingham, AL, USA,
Division of Pulmonary, Allergy, and Critical Care Medicine, University of Alabama at Birmingham (UAB), Birmingham, AL, USA,
Int J Chron Obstruct Pulmon Dis. 2018 Jul 27;13:2271-2278. doi: 10.2147/COPD.S165665. eCollection 2018.
Systemic corticosteroids (SC) are an integral part of managing acute exacerbations of COPD (AECOPD). However, the optimal dose and duration vary widely in clinical practice. We hypothesized that the use of a "PowerPlan" order set in the electronic health system (EHS) that includes a 5-day SC order would be associated with a reduced steroid dose and length of stay (LOS) for individuals hospitalized with AECOPD.
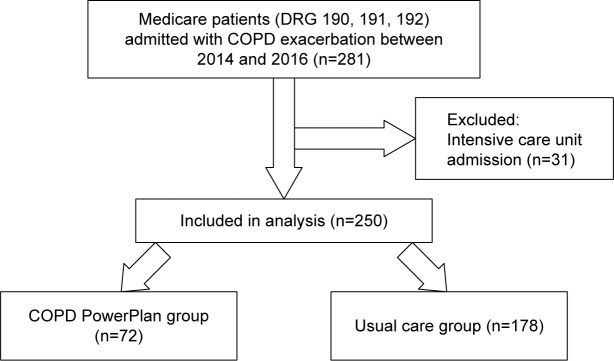
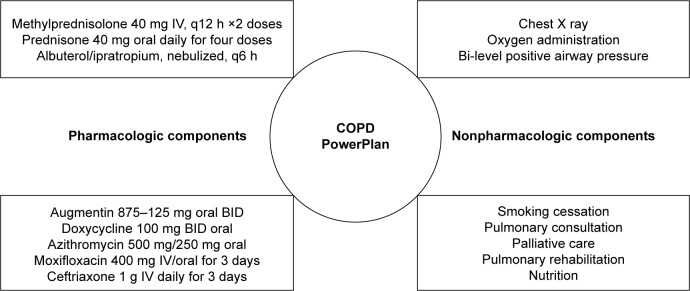
We conducted a retrospective cohort study of Medicare recipients discharged with an AECOPD diagnosis from our University Hospital from 2014 to 2016. Our EHS-based "COPD PowerPlan" order set included admission, laboratory, pharmacy, and radiology orders for managing AECOPD. The default SC option included intravenous methyl-prednisolone for 24 hours followed by oral prednisone for 4 days. The primary endpoint was the difference in cumulative steroid dose between the PowerPlan and the usual care group. Secondary endpoints included hospital LOS and readmission rates.
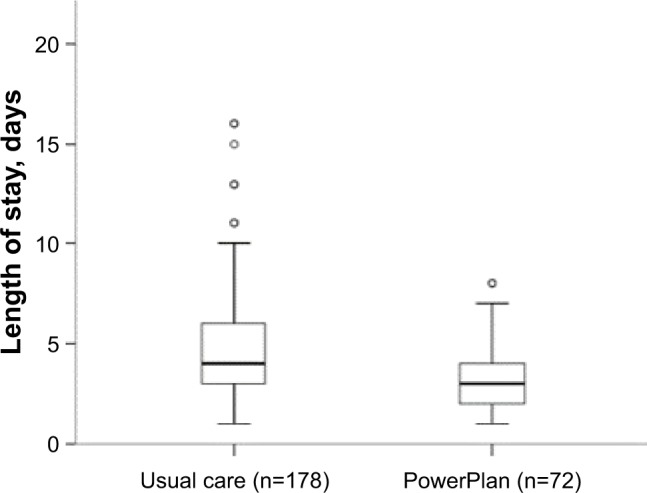
The 250 patients included for analysis were 62±11 years old, 58% male, with an FEV 55.1%±23.6% predicted. The PowerPlan was used in 72 (29%) patients. Cumulative steroid use was decreased by 31% in the PowerPlan group (420±224 vs 611±462 mg, <0.001) when compared with usual care. PowerPlan use was independently associated with decreased LOS (3 days; IQR 2-4 days vs 4 days; IQR 3-6 days, =0.022) without affecting 30- and 90-day readmission rates.
Use of a standardized EHS-based order set to manage AECOPD was associated with a reduction in steroid dose and hospital LOS.
全身用糖皮质激素(SC)是慢性阻塞性肺疾病急性加重期(AECOPD)治疗的重要组成部分。然而,在临床实践中,最佳剂量和疗程差异很大。我们假设,在电子健康系统(EHS)中使用包含5天SC医嘱的“PowerPlan”医嘱集,将使因AECOPD住院的患者的类固醇剂量和住院时间(LOS)减少。
我们对2014年至2016年从我校医院出院的诊断为AECOPD的医疗保险受益患者进行了一项回顾性队列研究。我们基于EHS的“COPD PowerPlan”医嘱集包括用于管理AECOPD的入院、实验室、药房和放射科医嘱。默认的SC选项包括静脉注射甲泼尼龙24小时,然后口服泼尼松4天。主要终点是PowerPlan组和常规治疗组之间累积类固醇剂量的差异。次要终点包括住院LOS和再入院率。
纳入分析的250例患者年龄为62±11岁,男性占58%,预测的第1秒用力呼气容积(FEV)为55.1%±23.6%。72例(29%)患者使用了PowerPlan。与常规治疗相比,PowerPlan组的累积类固醇使用量减少了31%(420±224 vs 611±462 mg,P<0.001)。使用PowerPlan与LOS缩短独立相关(3天;四分位间距2 - 4天 vs 4天;四分位间距3 - 6天,P = 0.022),且不影响30天和90天再入院率。
使用基于EHS的标准化医嘱集管理AECOPD与类固醇剂量减少和住院LOS缩短相关。