Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL; Center for Outcomes and Effectiveness Research and Education, Department of Medicine University of Alabama at Birmingham, Birmingham, AL; Lung Health Center, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL; Center for Palliative and Supportive Care, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL.
The Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine, Dartmouth College, Lebanon, NH.
Am J Med. 2020 Jul;133(7):817-824.e1. doi: 10.1016/j.amjmed.2019.11.024. Epub 2019 Dec 27.
End-of-life spending and healthcare utilization among older adults with COPD have not been previously described.
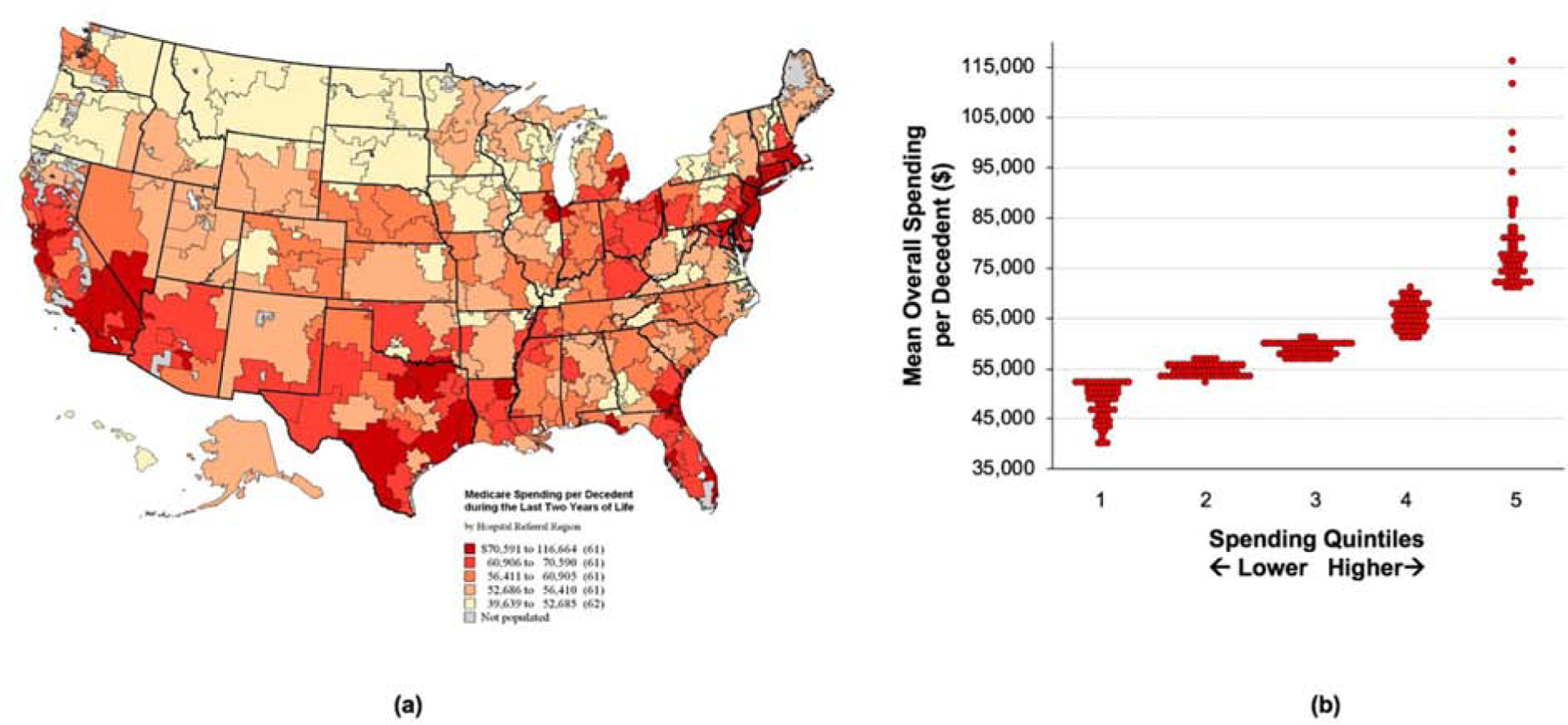
We examined data on Medicare beneficiaries aged 65 years or older with chronic obstructive pulmonary disease (COPD) who died during the period of 2013-2014. End-of-life measures were retrospectively reviewed for 2 years prior to death. Hospital referral regions (HRRs) were categorized into quintiles of age-sex-race-adjusted overall spending during the last 2 years of life. Geographic quintile variation in spending and healthcare utilization was examined across the continuum.
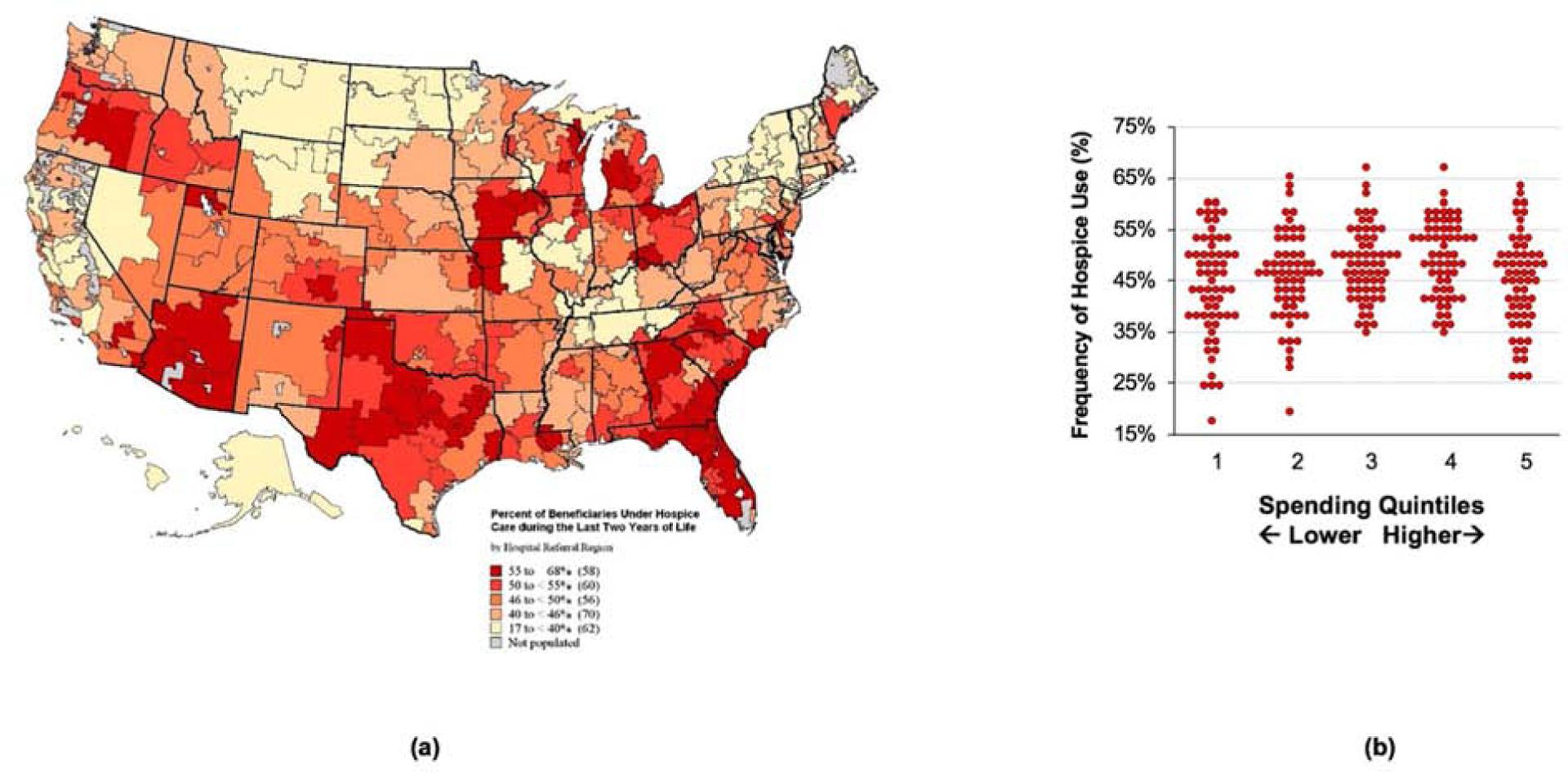
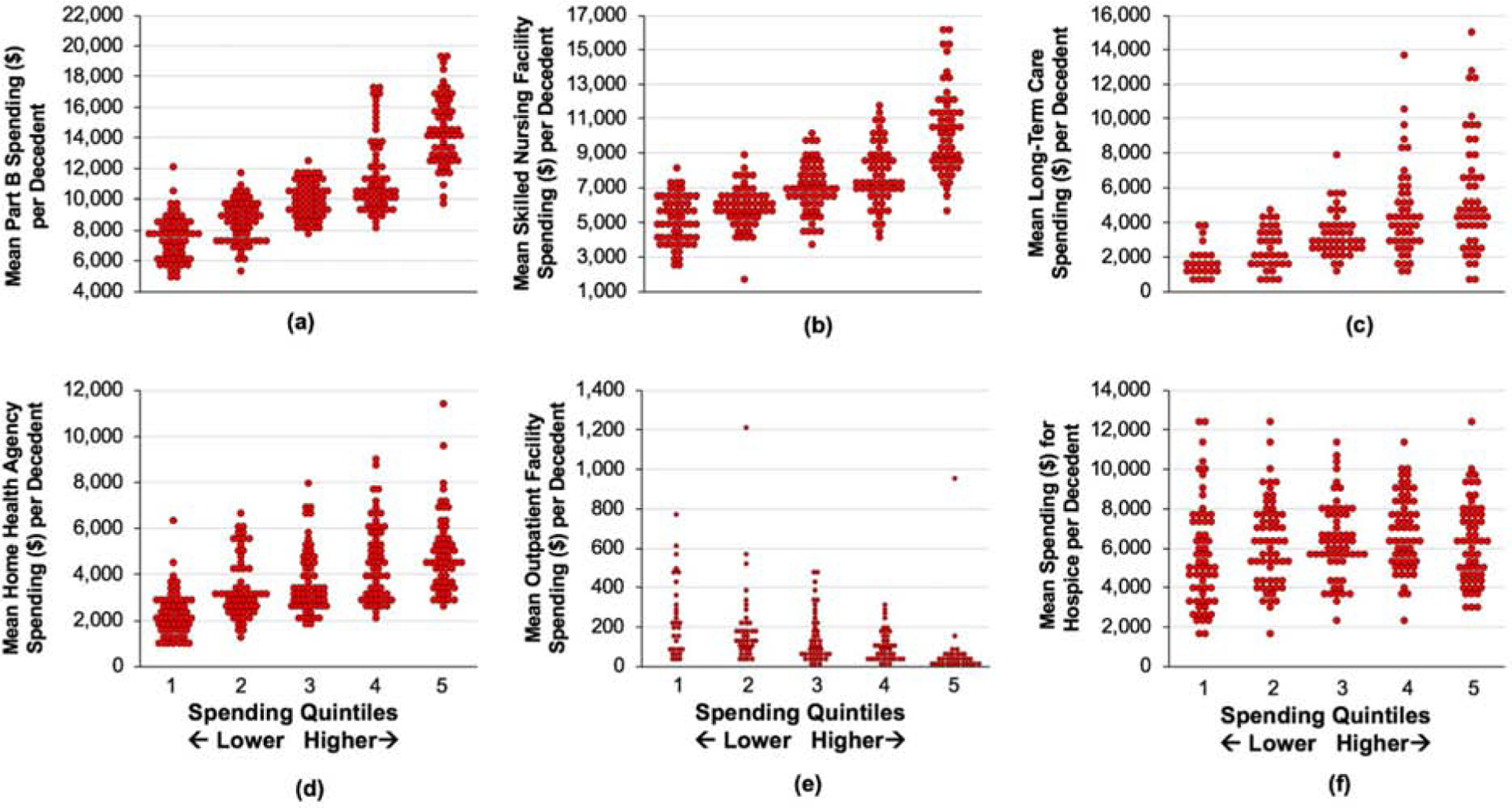
We investigated data on 146,240 decedents with COPD from 306 HRRs. Age-sex-race-adjusted overall spending per decedent during the last 2 years of life varied significantly nationwide ($61,271±$11,639 per decedent; range: $48,288±$3,665 to $79,453±$9,242). Inpatient care accounted for 40.2% of spending ($24,626±$6,192 per decedent). Overall, 82%±4% of decedents were admitted to the hospital for 13.7±3.1 days, and 55%±11% were admitted to an intensive care unit for 5.4±2.5 days. Compared with HRRs in the lowest spending quintile, HRRs in the highest spending quintile had a 1.5-fold longer hospital length of stay. Skilled nursing facilities accounted for 11.6% of spending ($7101±$2403 per decedent), and these facilities were utilized by 38%±7% of decedents for 18.7±4.9 days. Hospice accounted for 10.3% of spending ($6,307±$2,201 per decedent) and was utilized by 47%±9% of decedents for 39.7±14.8 days. Significant geographic variation in hospice utilization existed nationwide.
End-of-life spending and healthcare utilization among older adults with COPD varied substantially nationwide. Decedents with COPD frequently utilized acute care near the end of life. Hospice utilization was higher than expected, with significant geographic disparities.
目前尚未对老年 COPD 患者的临终支出和医疗保健利用情况进行描述。
我们对 2013-2014 年期间死亡的年龄在 65 岁及以上、患有慢性阻塞性肺疾病(COPD)的 Medicare 受益人数据进行了研究。对死亡前 2 年的临终措施进行了回顾性审查。将医院转介区(HRR)按生命最后 2 年的总调整后年龄-性别-种族支出分为五分位数。对临终和医疗保健利用情况的地理五分位变化进行了连续研究。
我们对来自 306 个 HRR 的 146240 名 COPD 死者的数据进行了调查。在生命的最后 2 年中,每位死者的调整后年龄-性别-种族总支出差异显著(每位死者 61271 美元±11639 美元;范围为 48288 美元±3665 美元至 79453 美元±9242 美元)。住院治疗占支出的 40.2%(每位死者 24626 美元±6192 美元)。总体而言,82%±4%的死者住院 13.7±3.1 天,55%±11%的死者入住重症监护病房 5.4±2.5 天。与支出最低的五分位 HRR 相比,支出最高的五分位 HRR 的住院时间长 1.5 倍。熟练护理设施占支出的 11.6%(每位死者 7101 美元±2403 美元),38%±7%的死者使用该设施 18.7±4.9 天。临终关怀占支出的 10.3%(每位死者 6307 美元±2201 美元),47%±9%的死者使用临终关怀 39.7±14.8 天。全国范围内,临终关怀的使用存在显著的地域差异。
老年 COPD 患者的临终支出和医疗保健利用情况在全国范围内差异很大。COPD 死者在生命的最后时刻经常使用急性护理。临终关怀的使用高于预期,存在显著的地域差异。