Russo Picasso María Fabiana, Vicens Jimena, Giuliani Carina, Jaén Ana Del Valle, Cabezón Carmen, Figari Marcelo, Gómez Saldaño Ana María, Figar Silvana
Department of Endocrinology, Metabolism and Nuclear Medicine, Hospital Italiano de Buenos Aires, Perón 4190 (1202), CABA, Argentina.
Epidemiology Section of the Department of Medicine & Department of Research, Hospital Italiano de Buenos Aires, Perón 4190 (1202), CABA, Argentina.
J Cancer Epidemiol. 2018 Jul 15;2018:8986074. doi: 10.1155/2018/8986074. eCollection 2018.
Two hypotheses attempt to explain the increase of thyroid cancer (TC) incidence: overdetection by excessive diagnostic scrutiny and a true increase in new cases brought about by environmental factors. Changes in the mechanism of detection and the risk of incidentally diagnosed TC could result in an increase of TC incidence.
Retrospective cohort study. We identified incident cases of TC from the pathological reports of patients in a HMO and review of clinical records. The results were analyzed in two periods: 2003-2007 and 2008-2012. Incidence rates expressed per 100,000 person-years (with 95% CI) and relative risk of incidence rates of incidental and nonincidental TC were estimated.
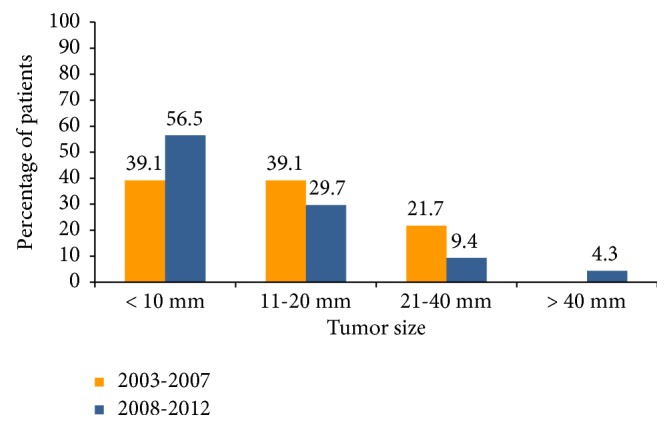
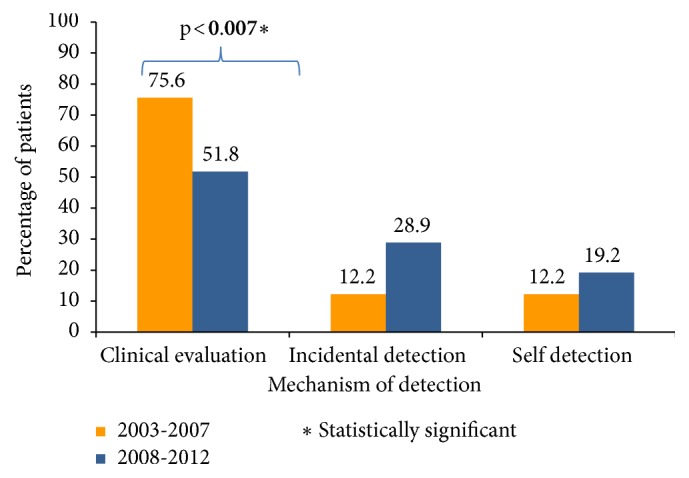
The relative risk of incidentally detecting a thyroid cancer in 2008-2012 compared to 2003-2007 was 6.06 (95%CI 1.84-20.04). Clinical evaluations detected 31 (75.6%) cancers in the period 2003-2007 and 70 (51.8%) cancers in the period 2008-2012 (p<0.007). Although tumor median size was significantly lower in the period 2008-2012 (10 vs. 14 mm, p<0.03), tumors greater than 40 mm (4.3%) were only present in 2008-2012. The female/male ratio decreased between analyzed periods from 8 (3-21) to 4 (3-7).
Our findings partially support the hypothesis of increased incidence due to overdetection but do not explain the changes in the increase of larger tumors and decrease in the female/male ratio, which could be secondary to the influence of unidentified environmental factors.
有两种假说试图解释甲状腺癌(TC)发病率的上升:一是过度诊断检查导致的过度检出,二是环境因素导致新发病例的真正增加。检测机制的变化以及偶然诊断出的TC的风险可能导致TC发病率上升。
回顾性队列研究。我们从一家健康维护组织(HMO)患者的病理报告和临床记录回顾中确定TC的发病病例。结果在两个时期进行分析:2003 - 2007年和2008 - 2012年。估计每10万人年的发病率(95%置信区间)以及偶然和非偶然TC发病率的相对风险。
与2003 - 2007年相比,2008 - 2012年偶然检测到甲状腺癌的相对风险为6.06(95%置信区间1.84 - 20.04)。临床评估在2003 - 2007年期间检测到31例(75.6%)癌症,在2008 - 2012年期间检测到70例(51.8%)癌症(p<0.007)。尽管2008 - 2012年期间肿瘤的中位大小显著更小(10对14毫米,p<0.03),但大于40毫米的肿瘤(4.3%)仅在2008 - 2012年出现。分析期间的男女比例从8(3 - 21)降至4(3 - 7)。
我们的研究结果部分支持了因过度检出导致发病率增加的假说,但无法解释较大肿瘤增加和男女比例下降的变化,这可能是未明确的环境因素影响的结果。