Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA; and.
Department of Medicine, University of Washington School of Medicine, Seattle, WA.
Blood Adv. 2018 Aug 14;2(15):2020-2028. doi: 10.1182/bloodadvances.2018021162.
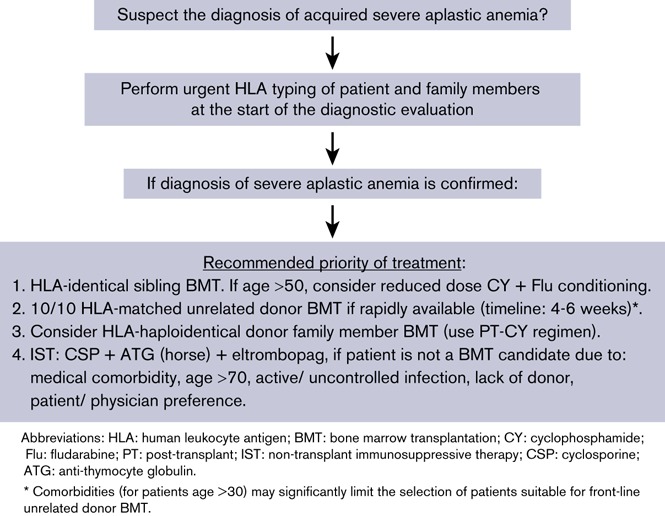
Treatment of severe aplastic anemia has improved significantly over the past 4 decades. This review will summarize the key areas of progress in the use of allogeneic hematopoietic cell transplantation and nontransplant immunosuppressive therapy (IST) for the treatment of aplastic anemia and then summarize the recommendations for first-line treatment. Based on recent data, we argue that guidelines for the initial treatment of patients with newly diagnosed severe aplastic anemia require revision. At the time of diagnosis, before beginning treatment, HLA typing should be done to identify a marrow donor among family members or in the unrelated donor registries, and a marrow transplant should be considered first-line therapy. The priority order of donor source for bone marrow transplantation is: (1) HLA-identical sibling, (2) HLA-matched unrelated donor, and (3) HLA-haploidentical donor if an HLA-matched unrelated donor is not rapidly available. Each of these donor marrow sources may be preferable to nontransplant IST. We make this recommendation because of the long-term persistent risk for disease relapse and secondary myelodysplastic syndrome or acute myeloid leukemia with the use of nontransplant IST for patients with aplastic anemia. In contrast, marrow transplantation is associated with high cure rates of aplastic anemia and a relatively low risk for graft-versus-host disease, with many patients now living for decades without the risk for disease recurrence or the development of clonal disorders. Implementation of this first-line treatment strategy will provide patients with severe aplastic anemia the best chance of long-term disease-free survival.
在过去的 40 年中,严重再生障碍性贫血的治疗有了显著改善。这篇综述将总结同种异体造血细胞移植和非移植免疫抑制疗法(IST)在治疗再生障碍性贫血方面的主要进展领域,然后总结一线治疗的建议。基于最近的数据,我们认为需要修订新诊断的严重再生障碍性贫血患者初始治疗的指南。在诊断时,开始治疗前,应进行 HLA 分型,以在家庭成员或无关供者登记处确定骨髓供者,并应首先考虑骨髓移植作为一线治疗。骨髓移植的供者来源的优先顺序为:(1)HLA 完全相同的同胞,(2)HLA 匹配的无关供者,(3)如果无法迅速获得 HLA 匹配的无关供者,则为 HLA 半相合供者。与非移植 IST 相比,这些供者骨髓来源中的每一种都可能更优。我们做出这一推荐是因为对于再生障碍性贫血患者,非移植 IST 的长期持续疾病复发和继发性骨髓增生异常综合征或急性髓系白血病的风险较高。相比之下,骨髓移植与较高的再生障碍性贫血治愈率和相对较低的移植物抗宿主病风险相关,许多患者现在可以数十年无疾病复发或克隆性疾病发展的风险生存。实施这一一线治疗策略将为严重再生障碍性贫血患者提供长期无病生存的最佳机会。