Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Division of Metabolic and Vascular Health, Warwick Medical School, University of Warwick, Coventry, UK; Clinical & Experimental Sciences, Faculty of Medicine, University of Southampton, Southampton General Hospital, Southampton, UK.
Nitric Oxide. 2018 Nov 1;80:52-60. doi: 10.1016/j.niox.2018.08.006. Epub 2018 Aug 13.
Endogenous nitric oxide (NO) may contribute to ischemic and anesthetic preconditioning while exogenous NO protects against ischemia-reperfusion (I/R) injury in the heart and other organs. Why those beneficial effects observed in animal models do not always translate into clinical effectiveness remains unclear. To mitigate reperfusion damage a source of NO is required. NO inhalation is known to increase tissue NO metabolites, but little information exists about the lifetime of these species. We therefore sought to investigate the fate of major NO metabolite classes following NO inhalation in mice in vivo.
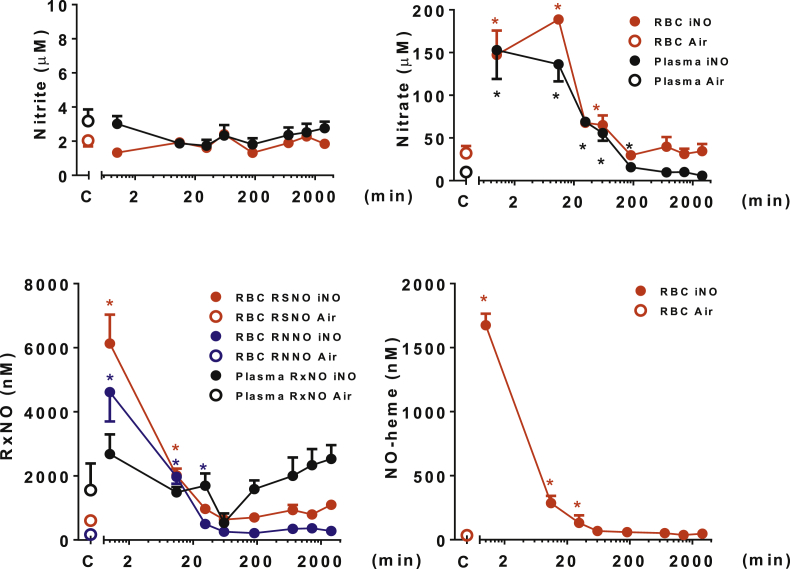
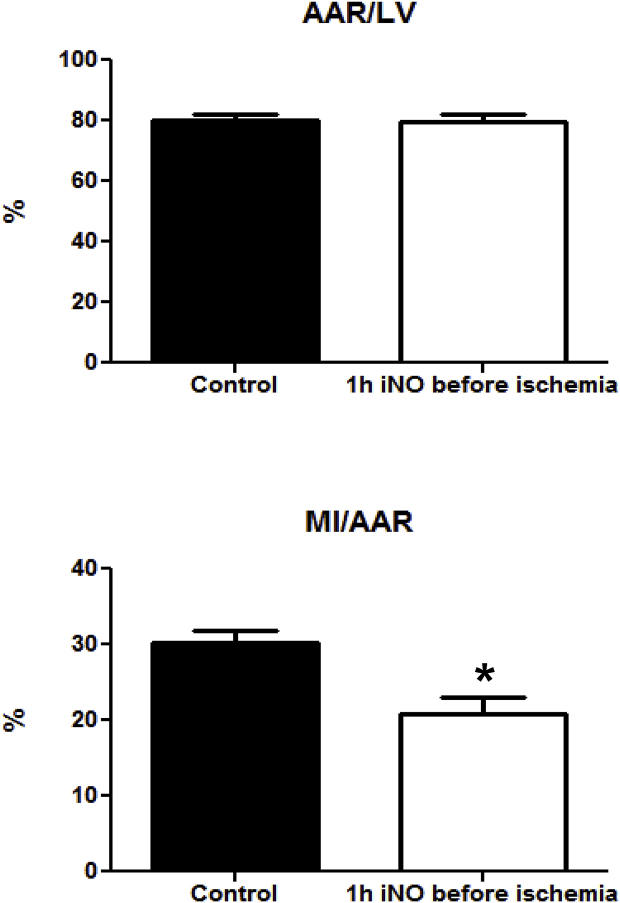
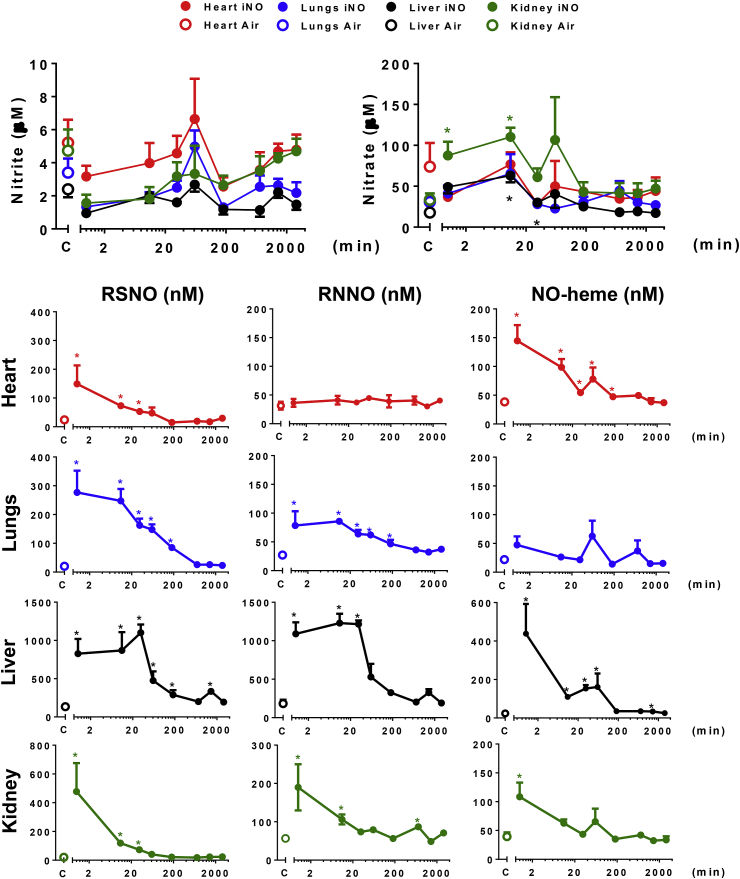
C57BL/6J mice were exposed to 80 ppm NO for 1 h. NO metabolites were measured in blood (plasma and erythrocytes) and tissues (heart, liver, lung, kidney and brain) immediately after NO exposure and up to 48 h thereafter. Concentrations of S-nitrosothiols, N-nitrosamines and NO-heme products as well as nitrite and nitrate were quantified by gas-phase chemiluminescence and ion chromatography. In separate experiments, mice breathed 80 ppm NO for 1 h prior to cardiac I/R injury (induced by coronary arterial ligation for 1 h, followed by recovery). After sacrifice, the size of the myocardial infarction (MI) and the area at risk (AAR) were measured.
After NO inhalation, elevated nitroso/nitrosyl levels returned to baseline over the next 24 h, with distinct multi-phasic decay profiles in each compartment. S/N-nitroso compounds and NO-hemoglobin in blood decreased exponentially, but remained above baseline for up to 30min, whereas nitrate was elevated for up to 3hrs after discontinuing NO breathing. Hepatic S/N-nitroso species concentrations remained steady for 30min before dropping exponentially. Nitrate only rose in blood, liver and kidney; nitrite tended to be lower in all organs immediately after NO inhalation but fluctuated considerably in concentration thereafter. NO inhalation before myocardial ischemia decreased the ratio of MI/AAR by 30% vs controls (p = 0.002); only cardiac S-nitrosothiols and NO-hemes were elevated at time of reperfusion onset.
Metabolites in blood do not reflect NO metabolite status of any organ. Although NO is rapidly inactivated by hemoglobin-mediated oxidation in the circulation, long-lived tissue metabolites may account for the myocardial preconditioning effects of inhaled NO. NO inhalation may afford similar protection in other organs.
内源性一氧化氮(NO)可能有助于缺血和麻醉预处理,而外源性 NO 可防止心脏和其他器官的缺血再灌注(I/R)损伤。为什么在动物模型中观察到的这些有益效果并不总是转化为临床效果尚不清楚。为了减轻再灌注损伤,需要 NO 的来源。已知吸入 NO 会增加组织 NO 代谢物,但关于这些物质的寿命知之甚少。因此,我们试图研究在体内吸入 NO 后,NO 主要代谢产物在小鼠体内的命运。
将 C57BL/6J 小鼠暴露于 80ppm 的 NO 中 1 小时。在 NO 暴露后立即和之后 48 小时内测量血液(血浆和红细胞)和组织(心脏、肝脏、肺、肾脏和大脑)中的 NO 代谢物。通过气相化学发光和离子色谱法定量测定 S-亚硝基硫醇、N-亚硝胺和 NO-血红素产物以及亚硝酸盐和硝酸盐的浓度。在单独的实验中,小鼠在心脏 I/R 损伤(冠状动脉结扎 1 小时,然后恢复)前吸入 80ppm 的 NO 1 小时。处死后,测量心肌梗死(MI)的大小和危险区(AAR)。
吸入 NO 后,下一个 24 小时内硝基/亚硝基水平恢复到基线,每个隔室都有明显的多相衰减曲线。血液中的 S/N-亚硝基化合物和 NO-血红蛋白呈指数下降,但在 30 分钟内仍高于基线,而硝酸盐在停止 NO 呼吸后 3 小时内仍升高。肝 S/N-亚硝基物种浓度在指数下降前稳定 30 分钟。硝酸盐仅在血液、肝脏和肾脏中升高;NO 吸入后即刻所有器官中的亚硝酸盐浓度均降低,但此后浓度波动较大。心肌缺血前吸入 NO 可使 MI/AAR 比值降低 30%(p=0.002);仅在再灌注开始时,心脏 S-亚硝基硫醇和 NO-血红素升高。
血液中的代谢物不能反映任何器官的 NO 代谢物状态。尽管 NO 会在循环中被血红蛋白介导的氧化快速失活,但长寿命的组织代谢物可能是吸入 NO 产生心肌预处理作用的原因。NO 吸入可能会为其他器官提供类似的保护。