1 Unit of Intensive Care, Pescara General Hospital, Pescara, Italy.
2 Unit of Clinical Pathology, Pescara General Hospital, Pescara, Italy.
Int J Immunopathol Pharmacol. 2018 Jan-Dec;32:2058738418792310. doi: 10.1177/2058738418792310.
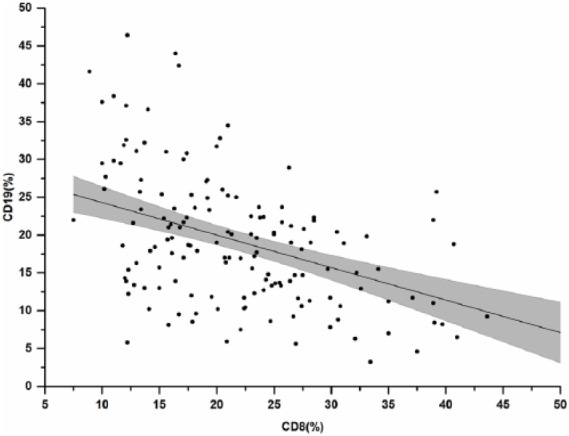
A better knowledge of factors predicting the development of sepsis in patients hospitalized in intensive care unit (ICU) might help deploy more targeted preventive and therapeutic strategies. In addition to the known clinical and demographic predictors of septic syndromes, in this study, we investigated whether measuring T and B lymphocyte subsets upon admission in the ICU may help individualize the prediction of ensuing sepsis during ICU stay. Between May 2015 and December 2016, we performed a prospective cohort study evaluating peripheral blood lymphocyte T-CD4+ (T-helper cells), T-CD8+ (cytotoxic T-cells), T-CD56 + (natural killer cells), and T-CD19+ (B-lymphocytes), using flow cytometry on blood samples collected 2 days after admission in the ICU. We enrolled 176 patients, 65.3% males, with mean age of 61.1 ± 15.4 years. At univariate analyses, higher percentages of CD19 B-cells were significantly associated with ensuing sepsis (20.5% (15.7-27.7)% vs 16.9% (11.3-22)%, P = 0.0001), whereas median interquartile range (IQR) proportions of CD4 T-cells (41.2% (33.4-50.6)% vs 40% (35-47)%, P = 0.5), CD8 T-cells (21.1% (15.8-28.2)% vs 19.6% (14.6-25.1)%, P = 0.2) and CD56 T-cells (1.7% (0.9-3.1)% vs 1.45% (0.7-2.3)%, P = 0.4) did not reveal any significant association. An unexpected, highly significant inverse correlation of CD8 T-cells and CD19 B-cells proportions, however, was observed, suggesting that patients with lower CD19 and higher CD8 proportions might be somehow protected from ensuing sepsis. We therefore studied the ability of the CD8/CD19 ratio to predict ensuing sepsis in our sample. In final models of multivariate logistic regression, the following independent associations were found: previous antibiotic exposure (odds ratio (OR): 3.8 (95% confidence interval (CI): 1.35-10.87), P = 0.01), isolation of at least one multi-drug resistant organism at any time during ICU stay (OR: 8.4 (95% CI: 3.47-20.6), P < 0.0001), decreasing age (OR: 0.9 (95% CI: 0.93-0.99), P = 0.02) and a CD8/CD19 ratio >2.2 (OR: 10.3 (95% CI: 1.91-55.36), P = 0.007). Our data provide preliminary evidence that immune characterization of critically ill patients on ICU admission may help personalize the prediction of ensuing sepsis during their ICU stay. Further polycentric evaluation of the true potential of this new tool is warranted.
更好地了解预测 ICU 住院患者发生脓毒症的因素,可能有助于部署更有针对性的预防和治疗策略。除了已知的临床和人口统计学预测因素外,在这项研究中,我们还研究了在 ICU 住院期间,入院时测量 T 和 B 淋巴细胞亚群是否有助于预测随后发生的败血症。2015 年 5 月至 2016 年 12 月,我们进行了一项前瞻性队列研究,使用流式细胞术评估入院后 2 天采集的外周血淋巴细胞 T-CD4+(辅助性 T 细胞)、T-CD8+(细胞毒性 T 细胞)、T-CD56+(自然杀伤细胞)和 T-CD19+(B 淋巴细胞)。我们纳入了 176 名患者,其中 65.3%为男性,平均年龄为 61.1±15.4 岁。单因素分析显示,较高的 CD19 B 细胞百分比与随后发生的败血症显著相关(20.5%(15.7-27.7)%比 16.9%(11.3-22)%,P=0.0001),而中位数四分位距(IQR)CD4 T 细胞比例(41.2%(33.4-50.6)%比 40%(35-47)%,P=0.5)、CD8 T 细胞(21.1%(15.8-28.2)%比 19.6%(14.6-25.1)%,P=0.2)和 CD56 T 细胞(1.7%(0.9-3.1)%比 1.45%(0.7-2.3)%,P=0.4)无显著相关性。然而,我们观察到 CD8 T 细胞和 CD19 B 细胞比例之间存在意外的、高度显著的负相关,这表明 CD19 较低和 CD8 较高的患者可能在某种程度上免受随后发生的败血症的影响。因此,我们研究了 CD8/CD19 比值在我们样本中预测随后发生败血症的能力。在多变量逻辑回归的最终模型中,发现了以下独立关联:先前的抗生素暴露(比值比(OR):3.8(95%置信区间(CI):1.35-10.87),P=0.01)、在 ICU 住院期间至少分离出一种多药耐药菌(OR:8.4(95% CI:3.47-20.6),P<0.0001)、年龄下降(OR:0.9(95% CI:0.93-0.99),P=0.02)和 CD8/CD19 比值>2.2(OR:10.3(95% CI:1.91-55.36),P=0.007)。我们的数据提供了初步证据,表明对 ICU 入院的危重病患者进行免疫特征分析可能有助于预测其 ICU 住院期间发生败血症的风险。需要进一步的多中心研究来评估这种新工具的真正潜力。