Kadia Tapan M, Cortes Jorge, Ravandi Farhad, Jabbour Elias, Konopleva Marina, Benton Christopher B, Burger Jan, Sasaki Koji, Borthakur Gautam, DiNardo Courtney D, Pemmaraju Naveen, Daver Naval, Ferrajoli Alessandra, Wang Xuemei, Patel Keyur, Jorgensen Jeffrey L, Wang Sa, O'Brien Susan, Pierce Sherry, Tuttle Carla, Estrov Zeev, Verstovsek Srdan, Garcia-Manero Guillermo, Kantarjian Hagop
Department of Leukemia, University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Leukemia, University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Lancet Haematol. 2018 Sep;5(9):e411-e421. doi: 10.1016/S2352-3026(18)30132-7. Epub 2018 Aug 13.
Front-line therapy for elderly or unfit patients with acute myeloid leukaemia (AML) remains unsatisfactory with poor outcomes and excessive toxicity. We studied a new low-intensity regimen of cladribine combined with low-dose cytarabine alternating with decitabine, aimed at improving outcomes in this population. Based on our previous experience, we hypothesised that this combination would be safe and more effective than current approaches with hypomethylating agents.
In this single-arm, open-label, single-centre phase 2 study, we enrolled patients aged 60 years or older with previously untreated AML or high-risk myelodysplastic syndrome who had adequate organ function and an Eastern Cooperative Oncology Group performance status of 2 or less. Patients were treated with cladribine plus low-dose cytarabine for two 28-day cycles alternating with decitabine for two 28-day cycles, for up to 18 cycles. Induction therapy (cycle 1) consisted of cladribine 5 mg/m intravenously over 1-2 h on days 1-5 and cytarabine 20 mg subcutaneously twice daily on days 1-10. Patients who had remission during this induction regimen moved on to consolidation therapy (cladribine 5 mg/m intravenously over 1-2 h on days 1-3 and cytarabine 20 mg twice daily on days 1-10, alternating with decitabine 20 mg/m intravenously on days 1-5). The primary outcome measure was disease-free survival. Secondary outcomes were overall survival, proportion of patients achieving complete response, proportion of patients achieving response, toxicity, and induction mortality. All treated patients were included in the analyses. This trial is ongoing and is registered with ClinicalTrials.gov, number NCT01515527.
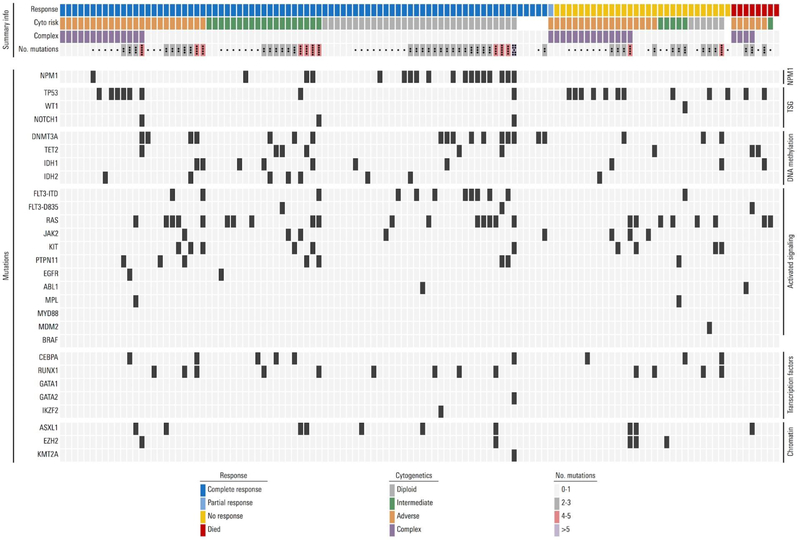
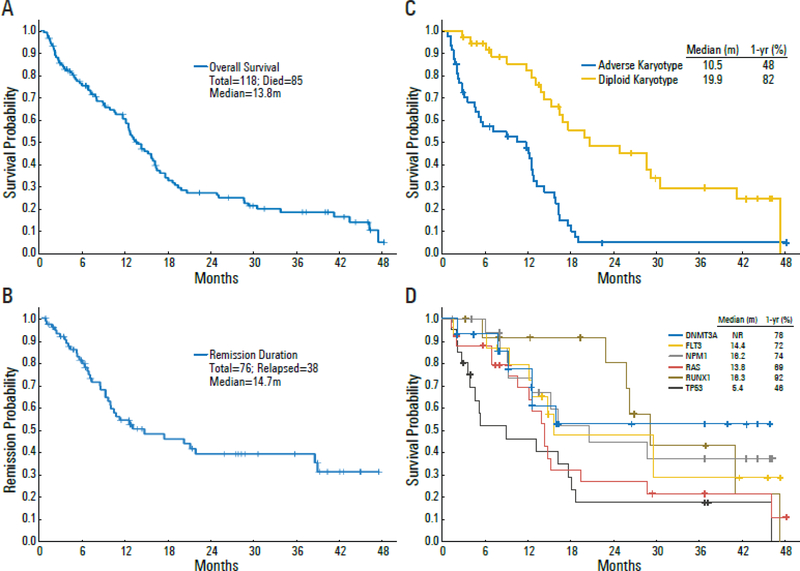
Between Feb 17, 2012, and July 6, 2017, 118 patients were enrolled and treated, among whom 48 (41%) had an adverse karyotype, 20 (17%) had therapy-related AML, 18 (15%) had treated secondary AML, and 20 (17%) had TP53 mutations. Median disease-free survival was 10·8 months (IQR 5·4-25·9). 80 (68%) patients achieved objective response: 69 (58%) achieved a complete response and 11 (9%) patients had complete response with incomplete count recovery. The median overall survival was 13·8 months (6·9-28·6). The regimen was well tolerated, with one (1%) death within the first 4 weeks and eight (7%) deaths within the first 8 weeks. The most common non-haematological adverse events of grade 3 or worse were infection (88 [75%] patients), elevated total bilirubin (26 [22%] patients), rash (13 [11%] patients), and nausea (13 [11%] patients).
The combination of cladribine and low-dose cytarabine alternating with decitabine appears to be a safe and highly effective regimen for the treatment of elderly or unfit patients with newly diagnosed AML. Further testing of this regimen is warranted, and could help to provide a new, effective option for reduced-intensity therapy in this population.
Part supported by the National Institutes of Health.
老年或身体状况不佳的急性髓系白血病(AML)患者的一线治疗效果仍不尽人意,预后差且毒性过大。我们研究了一种新的低强度方案,即克拉屈滨联合小剂量阿糖胞苷并与地西他滨交替使用,旨在改善该人群的治疗效果。基于我们之前的经验,我们假设这种联合方案将是安全的,并且比目前使用去甲基化药物的方法更有效。
在这项单臂、开放标签、单中心的2期研究中,我们纳入了年龄在60岁及以上、既往未接受治疗的AML或高危骨髓增生异常综合征患者,这些患者器官功能良好,东部肿瘤协作组体能状态评分为2分或更低。患者接受克拉屈滨加小剂量阿糖胞苷治疗两个28天周期,与地西他滨交替治疗两个28天周期,最多18个周期。诱导治疗(第1周期)包括在第1 - 5天静脉滴注克拉屈滨5mg/m²,持续1 - 2小时,以及在第1 - 10天皮下注射阿糖胞苷20mg,每日两次。在该诱导方案中获得缓解的患者进入巩固治疗(在第1 - 3天静脉滴注克拉屈滨5mg/m²,持续1 - 2小时,在第1 - 10天阿糖胞苷20mg每日两次,与在第1 - 5天静脉滴注地西他滨20mg/m²交替)。主要结局指标是无病生存期。次要结局包括总生存期、达到完全缓解的患者比例、达到缓解的患者比例、毒性和诱导期死亡率。所有接受治疗的患者均纳入分析。该试验正在进行中,并已在ClinicalTrials.gov注册,编号为NCT01515527。
在2012年2月17日至2017年7月6日期间,118例患者入组并接受治疗,其中48例(41%)具有不良核型,20例(17%)患有治疗相关AML,18例(15%)患有治疗相关性继发性AML,20例(17%)具有TP53突变。中位无病生存期为10.8个月(四分位间距5.4 - 25.9)。80例(68%)患者达到客观缓解:69例(58%)达到完全缓解,11例(9%)患者达到血细胞计数未完全恢复的完全缓解。中位总生存期为13.8个月(6.9 - 28.6)。该方案耐受性良好,在最初4周内有1例(1%)死亡,在最初8周内有8例(7%)死亡。最常见的3级或更严重的非血液学不良事件是感染(88例[75%]患者)、总胆红素升高(26例[22%]患者)、皮疹(13例[11%]患者)和恶心(13例[11%]患者)。
克拉屈滨与小剂量阿糖胞苷并与地西他滨交替使用的联合方案似乎是治疗老年或身体状况不佳的新诊断AML患者的一种安全且高效的方案。有必要对该方案进行进一步测试,这可能有助于为该人群的降低强度治疗提供一种新的有效选择。
部分由美国国立卫生研究院资助。