Anderson S, Rennke H G, Brenner B M
J Clin Invest. 1986 Jun;77(6):1993-2000. doi: 10.1172/JCI112528.
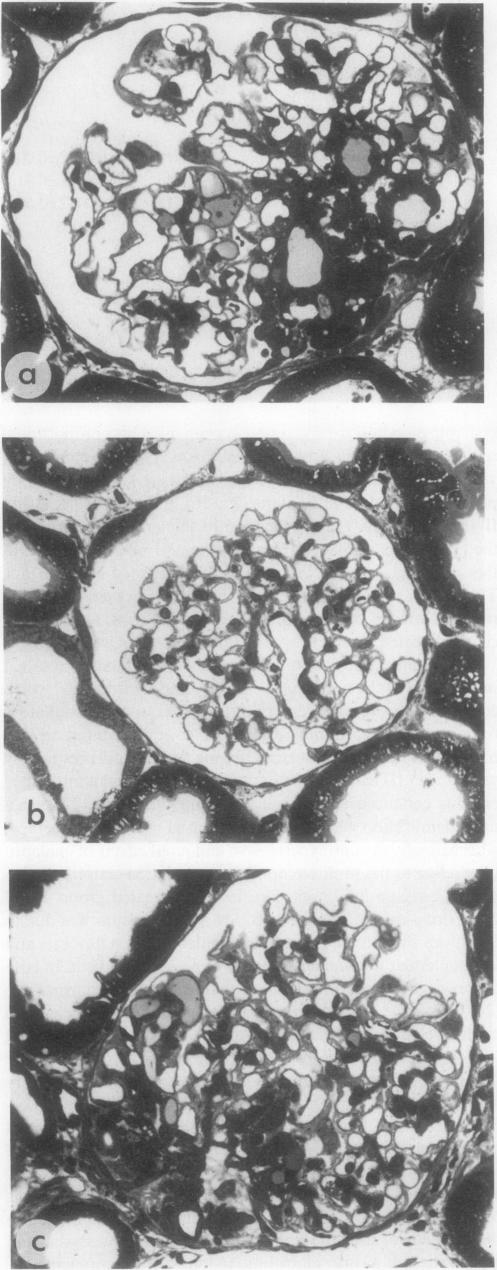
Micropuncture and morphologic studies were performed in six groups of male Munich-Wistar rats after removal of the right kidney and segmental infarction of two-thirds of the left kidney. Groups 1 and 4 received no specific therapy. Groups 2 and 5 were treated with the angiotensin I-converting enzyme inhibitor, enalapril, 50 mg/liter, in the drinking water. Groups 3 and 6 were treated with reserpine (5 mg/liter), hydralazine (80 mg/liter), and hydrochlorothiazide (25 mg/liter). All rats were fed standard chow. Groups 1-3 underwent micropuncture study 4 wk after renal ablation. Untreated group 1 rats exhibited systemic hypertension and elevation of the single nephron glomerular filtration rate (SNGFR) due to high average values for the mean glomerular transcapillary hydraulic pressure gradient (delta P) and glomerular plasma flow rate (QA). In group 2 rats, treatment with enalapril prevented systemic hypertension and maintained delta P at near-normal levels without significant reduction in SNGFR and QA. In contrast, triple drug therapy normalized systemic hypertension, but failed to lower delta P in group 3 rats. Groups 4-6 were followed for 12 wk after renal ablation. Untreated group 4 rats demonstrated continuous systemic hypertension, progressive proteinuria, and glomerular structural lesions, including mesangial expansion and frequent areas of segmental sclerosis. In group 5 rats, treatment with enalapril maintained systemic blood pressure at normal levels over the 12-wk period and dramatically limited the development of proteinuria and glomerular lesions. Despite equivalent systemic blood pressure control in group 6 rats, failure of triple drug therapy to control glomerular hypertension was associated with progressive proteinuria and glomerular lesions comparable to those seen in untreated group 4 rats. Thus, unless glomerular capillary hypertension is corrected, control of systemic blood pressure is insufficient to prevent progressive renal injury in rats with reduced renal mass.
对六组雄性慕尼黑 - 威斯塔大鼠进行了微穿刺和形态学研究,这些大鼠的右肾被切除,左肾三分之二发生节段性梗死。第1组和第4组未接受特殊治疗。第2组和第5组饮用含50 mg/升血管紧张素I转换酶抑制剂依那普利的水进行治疗。第3组和第6组用利血平(5 mg/升)、肼屈嗪(80 mg/升)和氢氯噻嗪(25 mg/升)进行治疗。所有大鼠均喂食标准饲料。第1 - 3组在肾切除术后4周进行微穿刺研究。未治疗的第1组大鼠出现全身性高血压,单个肾单位肾小球滤过率(SNGFR)升高,这是由于平均肾小球跨毛细血管液压梯度(ΔP)和肾小球血浆流速(QA)的平均值较高。在第2组大鼠中,依那普利治疗可预防全身性高血压,并使ΔP维持在接近正常水平,而SNGFR和QA无明显降低。相比之下,三联药物治疗使全身性高血压恢复正常,但未能降低第3组大鼠的ΔP。第4 - 6组在肾切除术后随访12周。未治疗的第4组大鼠表现出持续的全身性高血压、进行性蛋白尿和肾小球结构病变,包括系膜扩张和频繁的节段性硬化区域。在第5组大鼠中,依那普利治疗在12周期间将全身性血压维持在正常水平,并显著限制了蛋白尿和肾小球病变的发展。尽管第6组大鼠的全身性血压得到了同等控制,但三联药物治疗未能控制肾小球高血压,导致蛋白尿和肾小球病变进行性发展,并与未治疗第4组大鼠所见病变相当。因此,除非纠正肾小球毛细血管高血压,否则控制全身性血压不足以预防肾质量减少大鼠的进行性肾损伤。