Yi Lilan, Zhang Wei, Zhang Hongman, Shen Jie, Zou Jingwen, Luo Peng, Zhang Jian
Department of Oncology, Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, People's Republic of China,
Drug Des Devel Ther. 2018 Aug 7;12:2455-2466. doi: 10.2147/DDDT.S169627. eCollection 2018.
The clinical benefit of a selective cyclooxygenase-2 inhibitor, celecoxib, combined with anticancer therapy in advanced non-small-cell lung cancer (NSCLC) remains unclear. A meta-analysis was performed to address the efficacy and safety of celecoxib in patients with advanced NSCLC.
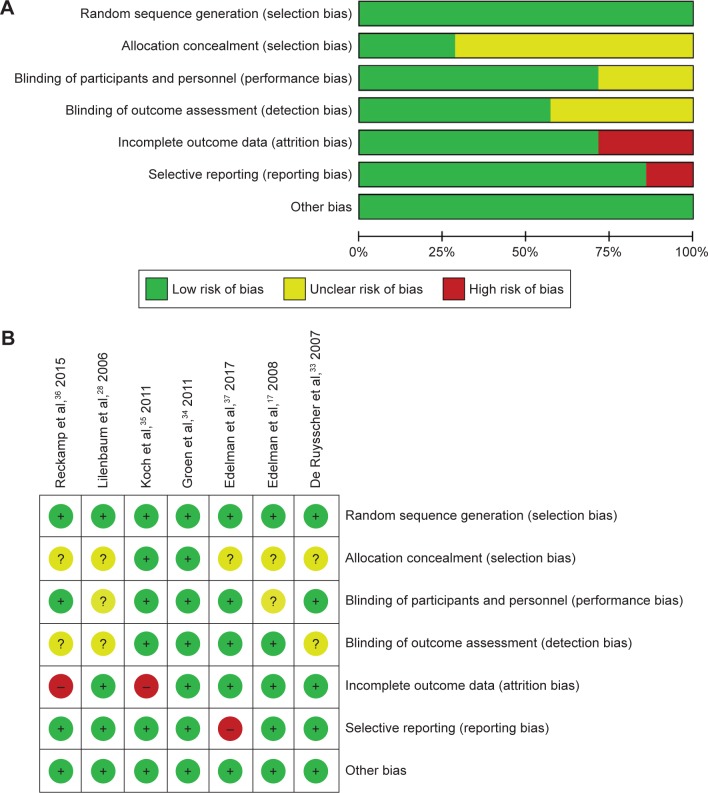
Three databases, including PubMed, EMBASE, and the Cochrane Library, were systematically searched for available literature until March 1, 2018. Data on tumor response rates, one-year survival, overall survival, progression-free survival, and toxicities were extracted from the included randomized clinical trials. Subgroup analysis was carried out according to the line of treatment. Review Manager 5.3 software was applied to conduct the meta-analysis.
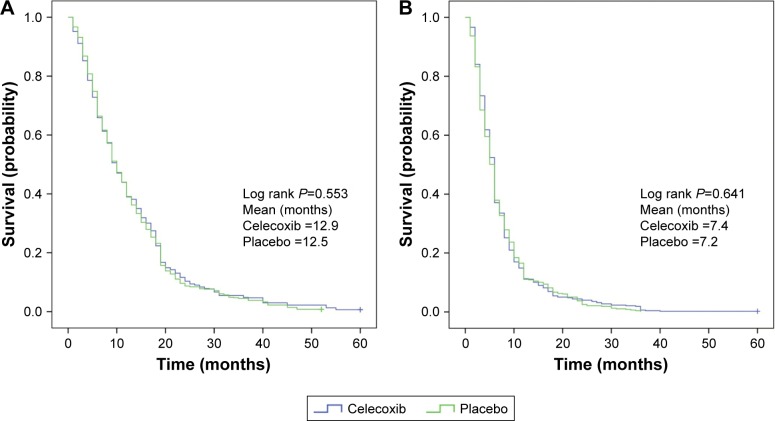
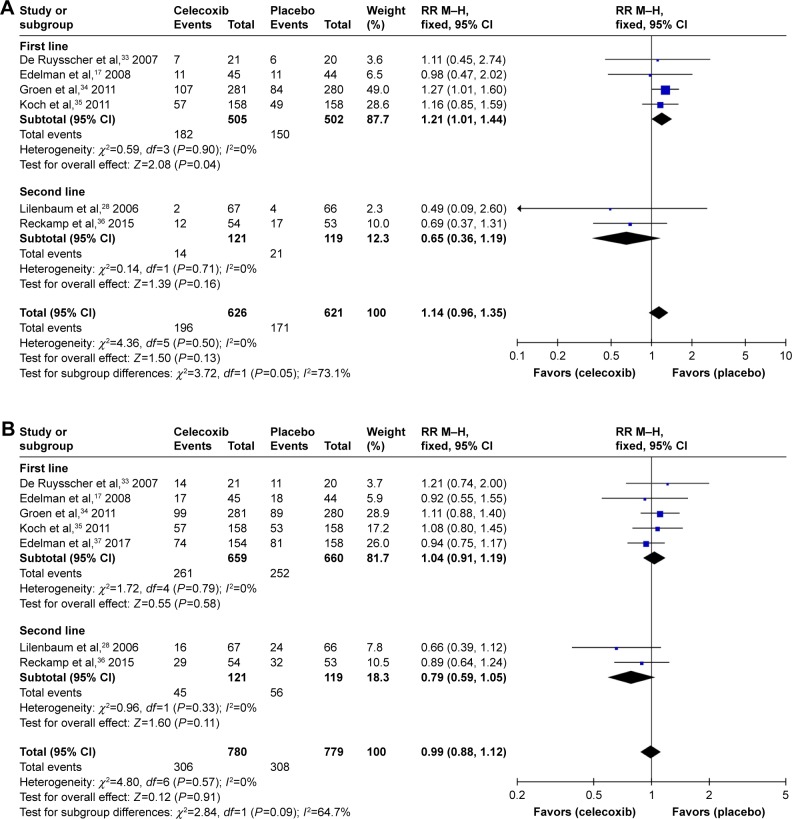
A total of 7 randomized controlled trials involving 1,559 patients with advanced NSCLC were enrolled for analysis. The pooled overall response rate (ORR) of celecoxib added to systemic therapy was not significantly improved (risk ratio [RR] =1.14, 95% CI =0.96-1.35, =0.13). Additionally, no differences were observed between the celecoxib and placebo groups regarding 1-year survival (RR =0.99, 95% CI =0.88-1.12, =0.91). Subgroup analysis showed that adding celecoxib to the first-line treatment significantly improved the ORR (RR =1.21, 95% CI =1.01-1.44, =0.04) and partial response rate (RR =1.26, 95% CI =1.01-1.58, =0.04). The aggregated Kaplan-Meier analysis found no significant difference between celecoxib and placebo regarding the 5-year overall survival (median, 12.9 vs 12.5 months, =0.553) and 5-year progression-free survival (median, 7.4 vs 7.2 months, =0.641). The increased RR of leukopenia (RR =1.25, 95% CI =1.03-1.50) and thrombocytopenia (RR =1.39, 95% CI =1.11-1.75) indicated that celecoxib increased hematologic toxicities (grade ≥III). However, celecoxib did not increase the related risks of thrombosis or embolism (RR =1.26, 95% CI =0.66-2.39) and cardiac ischemia (RR =1.16, 95% CI =0.39-3.44).
Celecoxib had no benefit on survival indices for advanced NSCLC but improved the ORR of first-line treatment. Additionally, celecoxib increased the rate of hematologic toxicities without increasing the risk of cardiovascular events.
选择性环氧化酶-2抑制剂塞来昔布联合抗癌疗法用于晚期非小细胞肺癌(NSCLC)的临床益处仍不明确。进行了一项荟萃分析以探讨塞来昔布用于晚期NSCLC患者的疗效和安全性。
系统检索了包括PubMed、EMBASE和Cochrane图书馆在内的三个数据库,以获取截至2018年3月1日的可用文献。从纳入的随机临床试验中提取肿瘤缓解率、一年生存率、总生存率、无进展生存率和毒性的数据。根据治疗线进行亚组分析。应用Review Manager 5.3软件进行荟萃分析。
共纳入7项涉及1559例晚期NSCLC患者的随机对照试验进行分析。添加塞来昔布至全身治疗的汇总总缓解率(ORR)未显著提高(风险比[RR]=1.14,95%可信区间[CI]=0.96-1.35,P=0.13)。此外,塞来昔布组和安慰剂组在1年生存率方面未观察到差异(RR=0.99,95%CI=0.88-1.12,P=0.91)。亚组分析显示,在一线治疗中添加塞来昔布显著提高了ORR(RR=1.21,95%CI=1.01-1.44,P=0.04)和部分缓解率(RR=1.26,95%CI=1.01-1.58,P=0.04)。汇总的Kaplan-Meier分析发现,塞来昔布和安慰剂在5年总生存率(中位数,12.9对12.5个月,P=0.553)和5年无进展生存率(中位数,7.4对7.2个月,P=0.641)方面无显著差异。白细胞减少症(RR=1.25,95%CI=1.03-1.50)和血小板减少症(RR=1.39,95%CI=1.11-1.75)的RR增加表明塞来昔布增加了血液学毒性(≥III级)。然而,塞来昔布并未增加血栓形成或栓塞(RR=1.26,95%CI=0.66-2.39)和心脏缺血(RR=1.16,95%CI=0.39-3.44)的相关风险。
塞来昔布对晚期NSCLC的生存指标无益处,但改善了一线治疗的ORR。此外,塞来昔布增加了血液学毒性发生率,而未增加心血管事件风险。