Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts.
Division of Gerontology, Department of Medicine, Beth Israel Deaconess Medical Center, Boston, Massachusetts.
J Am Geriatr Soc. 2018 Aug;66(8):1491-1498. doi: 10.1111/jgs.15418. Epub 2018 Aug 19.
To evaluate temporal trends and between-hospital variation in off-label antipsychotic medication (APM) use in older adults undergoing cardiac surgery.
Retrospective cohort study.
National administrative database including 465 U.S. hospitals.
Individuals aged 65 and older without known indications for APMs who underwent cardiac surgery from 2004 to 2014 (N=293,212).
Postoperative exposure to any APMs and potentially excessive dosing were examined. Hospital-level APM prescribing intensity was defined as the proportion of individuals newly treated with APMs in the postoperative period.
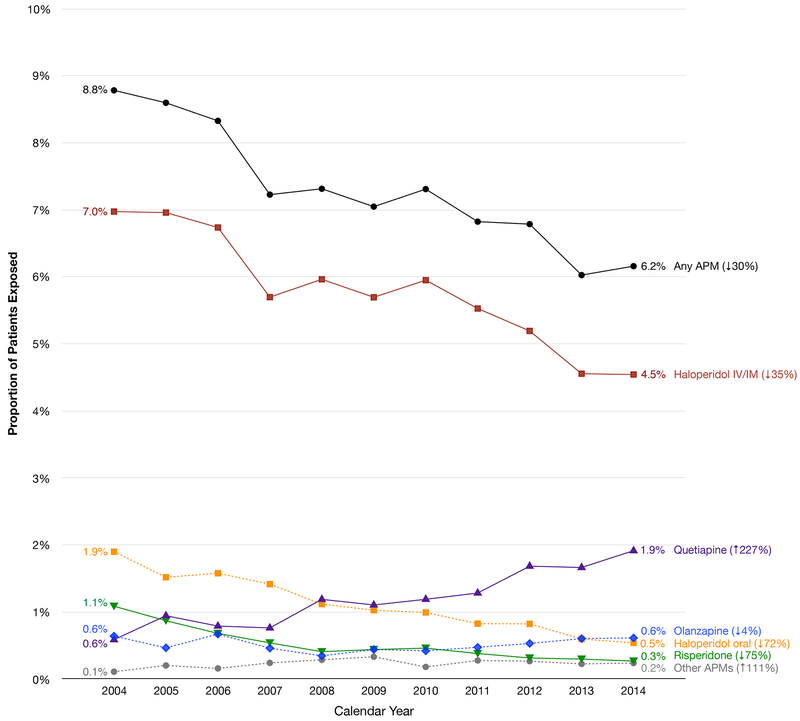
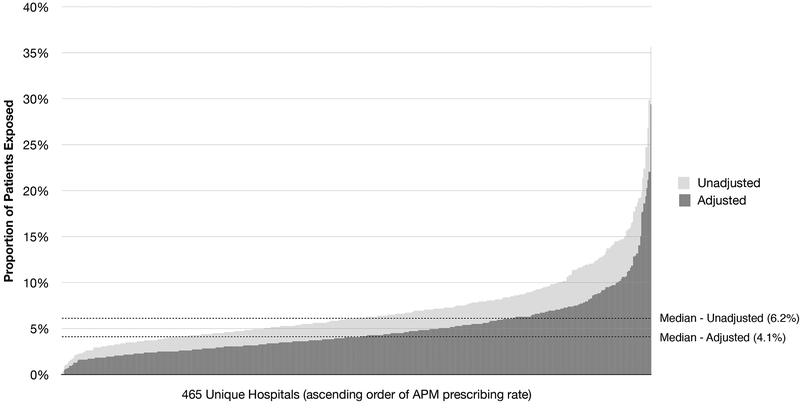
The rate of APM use declined from 8.8% in 2004 to 6.2% in 2014 (p<.001). Use of haloperidol (parenteral 7.0% to 4.5%, p<.001; oral: 1.9% to 0.5%, p<.001), and risperidone (1.1% to 0.3%, p<.001) declined, whereas quetiapine use tripled (0.6% to 1.9%, p=.03). Hospital APM prescribing intensity varied widely, from 0.3% to 35.6%, across 465 hospitals. Treated individuals at higher-prescribing hospitals were more likely to receive APMs on the day of discharge (highest vs lowest quintile: 15.1% vs 9.6%; p<.001) and for a longer duration (4.8 vs 3.7 days; p<.001) than those at lower-prescribing hospitals. Delirium was the strongest risk factor for APM exposure (odds ratio=9.73, 95% confidence interval=9.02-10.5), whereas none of the hospital characteristics were significantly associated. The rate of potentially excessive dosing declined (60.7% to 44.9%, p<.001), and risk factors for potentially excessive dosing were similar to those for any APM exposure.
Our findings suggest highly variable prescribing cultures and raise concerns about inappropriate use, highlighting the need for better evidence to guide APM prescribing in hospitalized older adults after cardiac surgery.
评估老年心脏手术患者中标签外使用抗精神病药物(APM)的时间趋势和医院间差异。
回顾性队列研究。
包括 465 家美国医院的国家行政数据库。
2004 年至 2014 年期间无已知 APM 适应证但接受心脏手术的 65 岁及以上个体(N=293212)。
术后暴露于任何 APM 和潜在过度剂量的情况。医院水平 APM 处方强度定义为术后新接受 APM 治疗的个体比例。
APM 使用率从 2004 年的 8.8%下降到 2014 年的 6.2%(p<.001)。氟哌啶醇(注射:7.0%至 4.5%,p<.001;口服:1.9%至 0.5%,p<.001)和利培酮(1.1%至 0.3%,p<.001)的使用率下降,而喹硫平的使用率增加了两倍(0.6%至 1.9%,p=.03)。465 家医院之间的 APM 处方强度差异很大,从 0.3%到 35.6%不等。在高处方医院接受治疗的个体在出院当天(最高五分位比最低五分位:15.1%比 9.6%;p<.001)和更长的时间(4.8 比 3.7 天;p<.001)接受 APM 的可能性更高。谵妄是 APM 暴露的最强危险因素(优势比=9.73,95%置信区间=9.02-10.5),而医院特征均无显著相关性。潜在过度剂量的发生率下降(60.7%至 44.9%,p<.001),潜在过度剂量的危险因素与任何 APM 暴露的危险因素相似。
我们的发现表明处方文化差异很大,并引起了对不适当使用的关注,这突出表明需要更好的证据来指导心脏手术后住院老年患者的 APM 处方。