From the Department of Anesthesiology.
Critical Illness, Brain Dysfunction, and Survivorship (CIBS) Center at Vanderbilt.
Anesth Analg. 2021 Sep 1;133(3):713-722. doi: 10.1213/ANE.0000000000005365.
Pharmacologic agents are frequently utilized for management of intensive care unit (ICU) delirium, yet prescribing patterns and impact of medication choices on patient outcomes are poorly described. We sought to describe prescribing practices for management of ICU delirium and investigate the independent association of medication choice on key in-hospital outcomes including delirium resolution, in-hospital mortality, and days alive and free of the ICU or hospital.
A retrospective study of delirious adult ICU patients at a tertiary academic medical center. Data were obtained regarding daily mental status (normal, delirious, and comatose), pharmacologic treatment, hospital course, and survival via electronic health record. Daily transition models were constructed to assess the independent association of previous day mental status and medication administration on mental status the following day and in-hospital mortality, after adjusting for prespecified covariates. Linear regression models investigated the association of medication administration on days alive and free of the ICU or the hospital during the first 30 days after ICU admission.
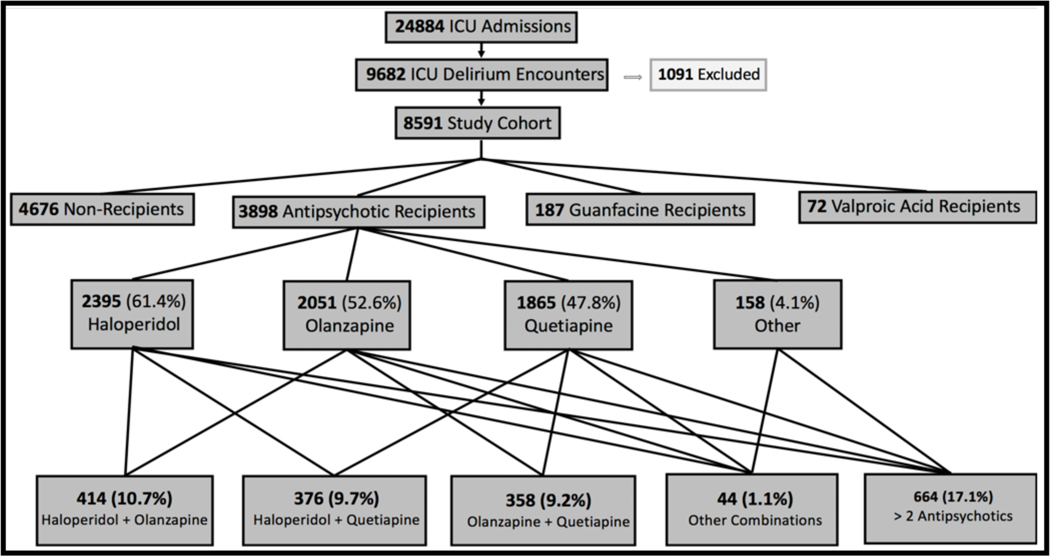
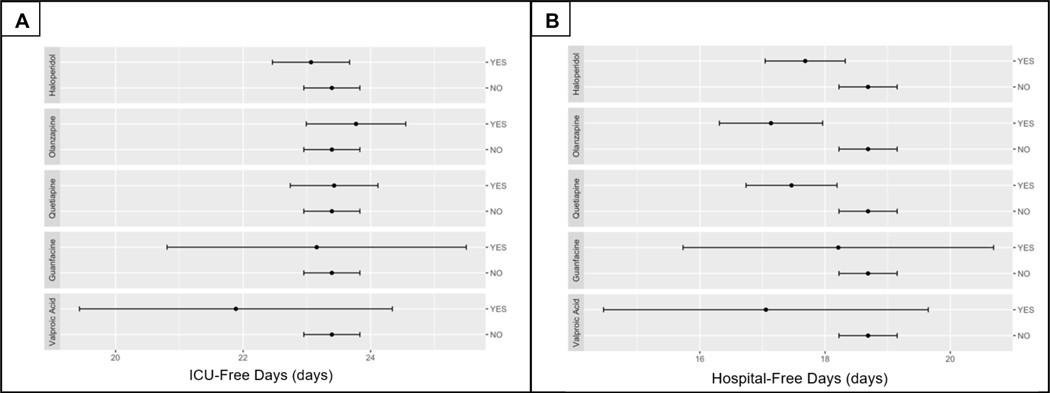
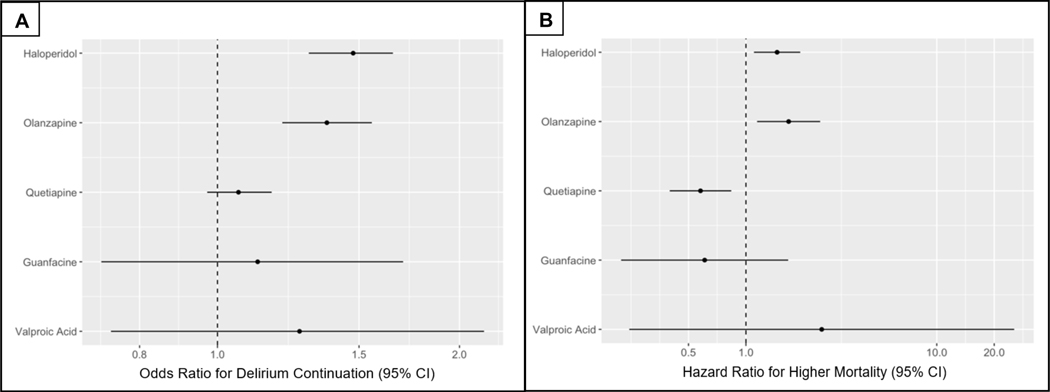
We identified 8591 encounters of ICU delirium. Half (45.6%) of patients received pharmacologic treatment for delirium, including 45.4% receiving antipsychotics, 2.2% guanfacine, and 0.84% valproic acid. Median highest Richmond Agitation-Sedation Scale (RASS) score was 1 (0, 1) in patients initiated on medications and 0 (-1, 0) for nonrecipients. Haloperidol, olanzapine, and quetiapine comprised >97% of antipsychotics utilized with 48% receiving 2 or more and 20.6% continued on antipsychotic medications at hospital discharge. Haloperidol and olanzapine were associated with greater odds of continued delirium (odds ratio [OR], 1.48; 95% confidence interval [95% CI], 1.30-1.65; P < .001 and OR, 1.37; 95% CI, 1.20-1.56; P = .003, respectively) and increased hazard of in-hospital mortality (hazard ratio [HR], 1.46; 95% CI, 1.10-1.93; P = .01 and HR, 1.67; 95% CI, 1.14-2.45; P = .01, respectively) while quetiapine showed a decreased hazard of in-hospital mortality (HR, 0.58; 95% CI, 0.40-0.84; P = .01). Haloperidol, olanzapine, and quetiapine were associated with fewer days alive and free of hospitalization (all P < .001). There was no significant association of any antipsychotic medication with days alive and free of the ICU. Neither guanfacine nor valproic acid were associated with in-hospital outcomes examined.
Pharmacologic interventions for management of ICU delirium are common, most often with antipsychotics, and frequently continued at hospital discharge. These medications may not portend benefit, may introduce additional harm, and should be used with caution for delirium management. Continuation of these medications through hospitalization and discharge draws into question their safety and role in patient recovery.
在重症监护病房(ICU)中,经常使用药物来治疗谵妄,但药物选择的处方模式和对患者预后的影响描述得很差。我们旨在描述管理 ICU 谵妄的处方实践,并研究药物选择对关键住院结局的独立关联,包括谵妄缓解、住院死亡率以及在 ICU 或医院存活的天数。
这是一项对一家三级学术医疗中心 ICU 中出现谵妄的成年患者进行的回顾性研究。通过电子病历获取关于每日神志状态(正常、谵妄和昏迷)、药物治疗、住院过程和存活情况的数据。构建每日过渡模型,以评估前一天的神志状态和药物管理对次日神志状态和住院死亡率的独立关联,同时调整了预设的协变量。线性回归模型调查了在 ICU 入院后的前 30 天内,药物管理对 ICU 或医院存活天数的关联。
我们确定了 8591 例 ICU 谵妄发作。一半(45.6%)的患者接受了治疗谵妄的药物治疗,包括 45.4%接受了抗精神病药物治疗,2.2%接受了胍法辛治疗,0.84%接受了丙戊酸治疗。在开始使用药物的患者中,中位数最高的 Richmond 躁动-镇静量表(RASS)评分为 1(0,1),而非接受者为 0(-1,0)。在使用的抗精神病药物中,氟哌啶醇、奥氮平和喹硫平占 97%以上,48%的患者接受了 2 种或更多药物,20.6%的患者在出院时仍继续使用抗精神病药物。氟哌啶醇和奥氮平与持续谵妄的可能性更大相关(比值比[OR],1.48;95%置信区间[95%CI],1.30-1.65;P <.001 和 OR,1.37;95%CI,1.20-1.56;P =.003),并增加了住院死亡率的风险(风险比[HR],1.46;95%CI,1.10-1.93;P =.01 和 HR,1.67;95%CI,1.14-2.45;P =.01),而喹硫平则降低了住院死亡率的风险(HR,0.58;95%CI,0.40-0.84;P =.01)。氟哌啶醇、奥氮平和喹硫平与存活天数和无住院天数减少相关(均 P <.001)。任何抗精神病药物与 ICU 存活天数或存活天数均无显著关联。胍法辛和丙戊酸均与研究的住院结局无关。
在 ICU 中治疗谵妄的药物干预措施很常见,最常使用的是抗精神病药物,并且经常在出院时继续使用。这些药物可能不会带来益处,可能会带来额外的危害,因此在治疗谵妄时应谨慎使用。这些药物在住院期间和出院后继续使用,这使得它们的安全性和在患者康复中的作用受到质疑。