Zhu Ling-Ling, Zhou Quan
VIP care ward, Division of Nursing, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, People's Republic of China.
Department of Pharmacy, the Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, People's Republic of China,
Infect Drug Resist. 2018 Aug 8;11:1105-1117. doi: 10.2147/IDR.S167616. eCollection 2018.
Sporadic studies in antimicrobial therapy have evaluated the effects of infusion rates on therapeutic and economic outcomes, and new findings may challenge the regular infusion regimen.
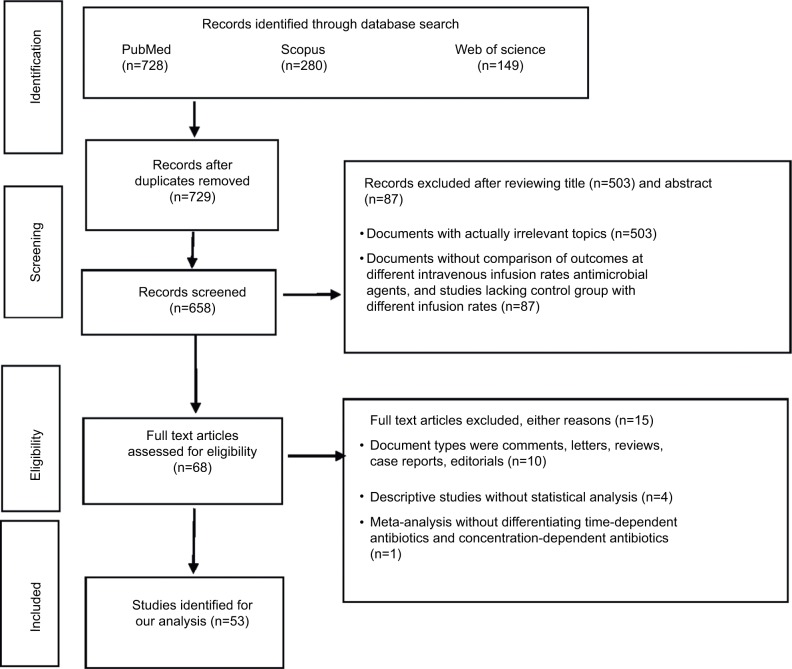
Focusing on studies comparing the outcomes of different infusion regimens, the relevant literature was identified by searching PubMed, Web of Science, and Scopus from January 1, 2013 to March 1, 2018. Papers were finally chosen using a PRISMA flowchart.
Antimicrobials with the superiority of prolonged infusion to standard infusion in terms of efficacy and safety include meropenem, doripenem, imipenem, cefepime, ceftazidime, piperacillin/tazobactam, linezolid, and vancomycin. The strategy of concomitantly reducing total daily dose and prolonging infusion time may cause treatment failure (eg, imipenem). Extended infusion of piperacillin/tazobactam has pharmacoeconomic advantage over standard infusion. Prolonged infusion of voriconazole is inferior to standard infusion because of lower efficacy caused by pharmacokinetic changes. Comparable outcomes following standard infusion and continuous infusion were observed with norvancomycin and nafcillin. Factors determining whether prolonged infusion has a benefit over standard infusion include MIC of bacterial pathogens, bacterial density, diagnosis, disease severity, total daily dose, and renal function.
To maximally preserve the effectiveness of current antimicrobials, effective interventions should be implemented to enhance the application of optimal infusion strategies. For reducing nephrotoxicity, prolonged infusion of meropenem is better than conventional infusion in neonates with Gram-negative late-onset sepsis, and continuous infusion of vancomycin is superior to intermittent infusion. For increasing efficacy, prolonged or continuous infusion of time-dependent antimicrobials (eg, meropenem, doripenem, imipenem, cefepime, ceftazidime, piperacillin/tazobactam, linezolid, and vancomycin) is an optimal choice. Nevertheless, such advantages may only be demonstrated in special clinical circumstances and special populations (eg, patients with a sequential organ failure assessment (SOFA) score≥9, respiratory tract infections, urinary or intra-abdominal infections, or infections caused by less susceptible pathogens would benefit from prolonged infusion of piperacillin/tazobactam).
抗菌治疗方面的零星研究评估了输注速率对治疗效果和经济结果的影响,新发现可能会对常规输注方案提出挑战。
聚焦于比较不同输注方案结果的研究,通过检索2013年1月1日至2018年3月1日期间的PubMed、Web of Science和Scopus来确定相关文献。最终使用PRISMA流程图选择论文。
在疗效和安全性方面,延长输注优于标准输注的抗菌药物包括美罗培南、多利培南、亚胺培南、头孢吡肟、头孢他啶、哌拉西林/他唑巴坦、利奈唑胺和万古霉素。同时降低每日总剂量并延长输注时间的策略可能会导致治疗失败(如亚胺培南)。哌拉西林/他唑巴坦延长输注在药物经济学方面优于标准输注。伏立康唑延长输注因药代动力学变化导致疗效降低而劣于标准输注。去甲万古霉素和萘夫西林在标准输注和持续输注后的结果相当。决定延长输注是否优于标准输注的因素包括细菌病原体的最低抑菌浓度、细菌密度、诊断、疾病严重程度、每日总剂量和肾功能。
为最大程度地保留当前抗菌药物的有效性,应实施有效干预措施以加强最佳输注策略的应用。为降低肾毒性,对于革兰阴性迟发性败血症新生儿,美罗培南延长输注优于传统输注,万古霉素持续输注优于间歇输注。为提高疗效,时间依赖性抗菌药物(如美罗培南、多利培南、亚胺培南、头孢吡肟、头孢他啶、哌拉西林/他唑巴坦、利奈唑胺和万古霉素)的延长或持续输注是最佳选择。然而,这些优势可能仅在特殊临床情况和特殊人群中得到体现(例如,序贯器官衰竭评估(SOFA)评分≥9的患者、呼吸道感染、泌尿系统或腹腔内感染,或由较难敏感病原体引起的感染,可能会从哌拉西林/他唑巴坦延长输注中获益)。