Zhou Junwen, Millier Aurélie, Toumi Mondher
Public Health Department, Aix-Marseille University, Marseille, France.
Health Economics and Outcomes Research Department, Creativ-Ceutical, Paris, France.
J Mark Access Health Policy. 2018 Aug 14;6(1):1508272. doi: 10.1080/20016689.2018.1508272. eCollection 2018.
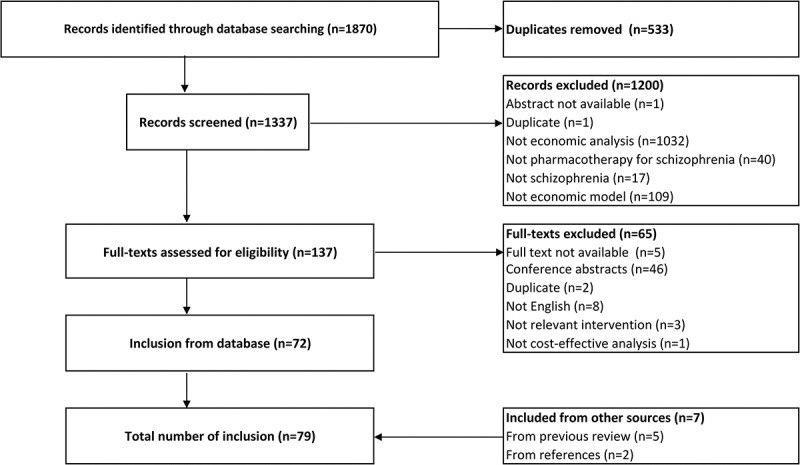
: Economic models are broadly used in the economic evaluation of antipsychotics in schizophrenia. Our objective was to summarize the structure of these models. : Model-based economic evaluations of antipsychotics in schizophrenia were identified through Medline and Embase. General information was extracted including analysis type, model type, perspective, population, comparator, outcome, and timeframe. Model-specific structures for decision tree (DT), cohort- and patient-level Markov model (CLMM, PLMM), and discrete-event simulation (DES) models were extracted. : A screen of 1870 records identified 79 studies. These were mostly cost-utility analyses (n = 48) with CLMM (n = 32) or DT models (n = 29). They mostly applied payer perspective (n = 68), focused on general schizophrenia for relapse prevention (n = 73), compared pharmacotherapies as first-line (n = 71), and evaluated incremental cost per quality-adjusted life year (QALY) gained (n = 40) with a 1-year (n = 32) or 5-year (n = 26) projection. DT models progressed with the branching points of response, relapse, discontinuation, and adherence. CLMM models transitioned between disease states, whereas PLMM models transitioned between adverse event states with/without disease state. DES models moved forward with times to remission, relapse, psychiatrist visit, and death. : A pattern of pharmacoeconomic models for schizophrenia was identified. More subtle structures and patient-level models are suggested for a future modelling exercise.
经济模型广泛应用于精神分裂症抗精神病药物的经济学评价。我们的目的是总结这些模型的结构。
通过医学文献数据库(Medline)和荷兰医学文摘数据库(Embase)检索精神分裂症抗精神病药物基于模型的经济学评价。提取一般信息,包括分析类型、模型类型、视角、人群、对照、结局和时间范围。提取决策树(DT)、队列水平和患者水平马尔可夫模型(CLMM、PLMM)以及离散事件模拟(DES)模型的特定模型结构。
筛查1870条记录后确定了79项研究。这些大多是成本效用分析(n = 48),采用CLMM(n = 32)或DT模型(n = 29)。它们大多采用支付方视角(n = 68),关注一般精神分裂症的复发预防(n = 73),比较一线药物治疗(n = 71),并评估每获得一个质量调整生命年(QALY)的增量成本(n = 40),预测期为1年(n = 32)或5年(n = 26)。DT模型根据反应、复发、停药和依从性的分支点推进。CLMM模型在疾病状态之间转换,而PLMM模型在有/无疾病状态的不良事件状态之间转换。DES模型根据缓解、复发、精神科就诊和死亡时间推进。
确定了精神分裂症药物经济学模型的模式。建议在未来的建模工作中采用更精细的结构和患者水平模型。